 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
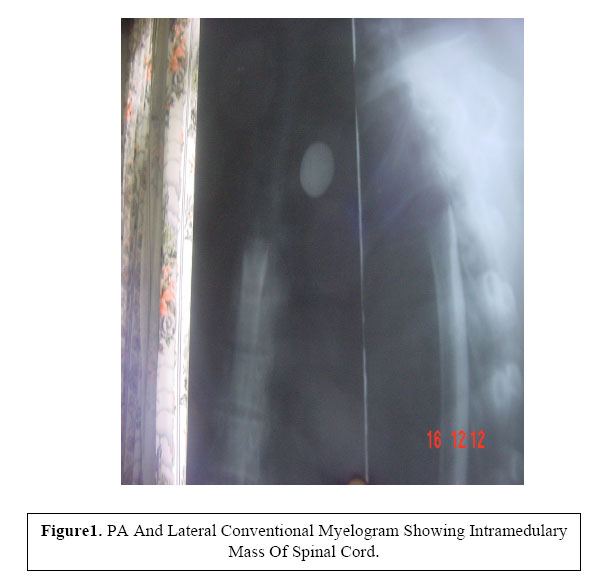
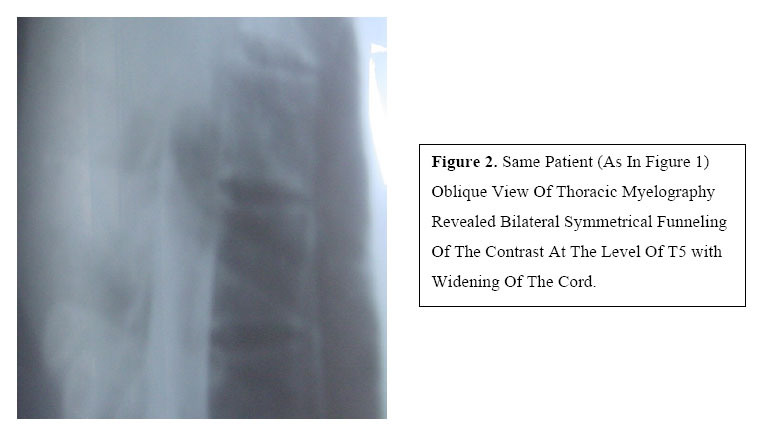
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 56-60 Intramedullary Cavernous Haemangioma Of Spinal Cord: A case report and Literature Review 1Tadios Muni M.D, 2Hagos Biluts M.D. 1Senior consultant Neurosurgeon,2Expert medical Specialist General surgeon. Code Number: js04040 A 27-year-old female patient presented with a 9-month history of back pain, trunk pain and progressive weakness of the lower limbs followed by incontinence of urine. Relevant literature reviewed, and treatment of the patient discussed. Thoracic myelography done showed bilateral symmetrical funnelling of the contrast at the level of T5 with widening of the spinal cord, which are typical characteristics of an intramedullary mass of spinal cord. T2-T6 Laminectomy was done. Near total excision of a 4 by 2.5 cm intradural, intramedulary bluish black, necrotic, fragile mass extending from T3-T5 was performed, and patient put on intensive physiotherapy. Histopathology revealed a cavernous haemangioma of spinal cord. In conclusion, even though cavernous haemangiomas of the spinal cord are extremely rare, they should be considered as a differential diagnosis in patients with progressive deterioration of spinal cord function. Total excision of the lesion is the current treatment modality. Introduction Haemangiomas are congenital vascular malformations, not true neoplasms, consisting of vessels reminiscent of embryonic capillaries or veins1,2,3 , that may present in any part of the body, but is particularly common in vertebral bodies, eye and orbit, brain and liver4 . Histologically haemangiomas are classically classified into capillary, cavernous and mixed types according to vessel size. Capillary haemangioma consists of capillaries with a sparse fibrous stroma, whereas cavernous haemangiomas are large dilated, bloodfilled spaces lined by flat endothelium4,5,6,7 . Cavernous haemangiomas are vascular hamartomas and occur throughout the neuroaxis8- 12 . They are more common in cerebral hemispheres and some in brain stem. Spinal cavernous malformations occur most commonly in vertebrae and may extend into extradural spinal canal. Intradural and extradural cavernomas have also been reported13 . Intramedullary haemangioma are extremely rare14,15 . The current Treatment of cavernous angiomas consists of total excision whenever possible7, 9,14,15,20 . In this review, a case of intradural intramedullary cavernous haemangioma that presented at Tikur Anbessa Hospital is presented and management of the condition discussed. Case Report A 27-year-old female patient presented with a 9- month history of back pain, and bilateral numbness of the lower limbs. The pain was dull, localized and was initially tolerable but latter on started to worsen radiating to both thighs and lower extremities. Three months latter, she started to develop gradual progressive weakness of the left lower limb first, followed by weakness of the right lower limb. Finally, the patient could walk only a few steps using walker. She also had burning sensation of both thighs and tingling sensation of both toes. Moreover, patient had occasional intermittent incontinence to urine. On neurological examinations the power on both lower extremities was grade 2/5 on MRI scale, deep tendon reflexes were brisk, had clasp knife type of tone (spastic) bilaterally and up going babiniski. Pain and touch sensations were completely lost on right lower limb and patchy sensory loss on the left side. Sensory level was at T6.Rest of the neurological as well as systemic examinations were non-contributory. Her routine haematological and biochemical parameters were within normal ranges. Chest roentgenogram and Thoracic dorsal roentgenogram were non-revealing. Thoracic myelography revealed bilateral symmetrical funnelling of the contrast at the level of T5 with widening of the cord, conclusion being intradural intramedulary mass of spinal cord (Figure 1, 2,). This patient underwent T2-T6 laminectomy. Myelotomy was done directly over the bluish black looking discoloration of the spinal cord. A 4x2.5cm bluish black, necrotic, fragile mass that is in continuity with the cord, extending from T3-T5 was removed, and the mass was nearly excised completely. Histophathological examinations of the mass revealed a focal hydropic changes partially necrotic vascular proliferation lined by bland endothelial cells, and large blood spaces, which is characteristics of cavernous haemangioma of the spinal cord. Patient started on intensive physiotherapy and showed gradual progressive improvement on subsequent follow up period. Discussion Haemangiomas are congenital vascular malformations, not true neoplasms1,2,3. Hitologically, haemangiomas are divided in to capillary, cavernous and mixed types, depending on the dominant vessel size at microscopy7,8. Capillary haemangiomas are the more common form and consists of capillary-sized vessels lined with flattened endothelium separated by a collageneous stroma whereas cavernous haemangiomas are large dilated-blood filled spaces lined by flat endothelium4,7,8. Intramedullary cavernous malformations of spinal cord occur more frequently in females with approximate ratio of 2:1. In general, the presentation is in the 3rd to 6th decades of life with progressive Paraparesis, sensory loss, frequently associated pain13,22. It may be indistinguishable from chronic progressive radiculomyelopathy. These varied manifestations are attributed to their variable size, which may vary from few millimetres to several centimetres. Acute symptoms are probably caused by new haemorrhages within or around the lesion. Slowly progressive course of the haemangioma may be due to local pressure effects on adjoining spinal cord and or repeated episodes of bleeding. Since the haemorrhage in cavernous haemangioma is venous and at low pressure, the presentation is not as dramatic as with arterial, bleed22. Incidental asymptomatic lesions have also been reported. The neurological deterioration may have sometimes-variable degree of recovery although most patients exhibit a gradual clinical decline22. On histopathological correlation, four major clinical patterns have been defined: a) Acute episodes of step-wise deterioration with small but repeated haemorrhages or with thrombosis of the malformed vessels. b) Slow progression due to progressive enlargement of the cavernoma eventually with thickening of the sinusoidal vessels and gradual thrombosis. c) Acute onset with rapid deterioration due to intraparenchymal haemorrhage. d) Acute onset with gradual decline attributable to altered microcirculation due to intraparenchymal haemorrhage23. The present case had acute onset with gradual deterioration of neurological function, attributable to altered microcirculation due to intraparenchymal haemorrhage23. Intramedullary haemangioma are extremely rare14,15. Cavernous haemangioma are angiographically occult16,17. MRI is diagnostic18. Radiologically, they resemble other vascular spinal cord tumour bony vertebral tumours and other intramedullary cord tumours19. We employed myelography, and revealed bilateral symmetrical funnelling of the contrast material at T5 level with widening of the cord. The current Treatment of cavernous angioma consists of total excision7,9,14,15,20. Zentner J et al15 and Vaquero J et al16 stated that Treatment of Cavernous haemangioma is surgical but there are only a few reports of complete surgical excision14,15. Total surgical resection under high magnification using microsurgical techniques is a procedure of choice for the management of Symptomatic intramedullary cavernous angioma26, and for patients with progressive neurological deficit to avert subsequent lesion enlargement or repeated haemorrhage25. Dissection must be performed by Making myelotomy directly over the bluish discoloration of lesion must perform dissection and limited to surrounding haemosiderine stained gliotic plane to avoid injury to normal surrounding neural tissue. Subtotal removal may lead to reappearance of symptoms and continued progressive deterioration because of bleeding from residual malformation22,27. Radio surgery has no role in the treatment of cavernous angioma21. Conclusion Cavernous haemangioma of spinal cord should be suspected in the differential diagnosis of patients with progressive and stepwise deterioration of spinal cord function. Precise diagnosis and timely treatment of cavernous haemangioma of spinal cord is mandatory to avoid misdiagnosis and resultant over treatment of this benign lesion. Total excision of symptomatic intrameduary cavernous haemangioma of the spinal cord is the treatment of choice to prevent further recurrence, bleeding into the cord and progressive neurological deterioration of the legs and sphincter functions. Acknowledgement We thank Dr. Miliard Derebew for taking photographs and Department of surgery for creating fertile working environment. Reference
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04040f2.jpg] [js04040f1.jpg] |
| |||||||||

{kind=link}
{kind=link}