 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
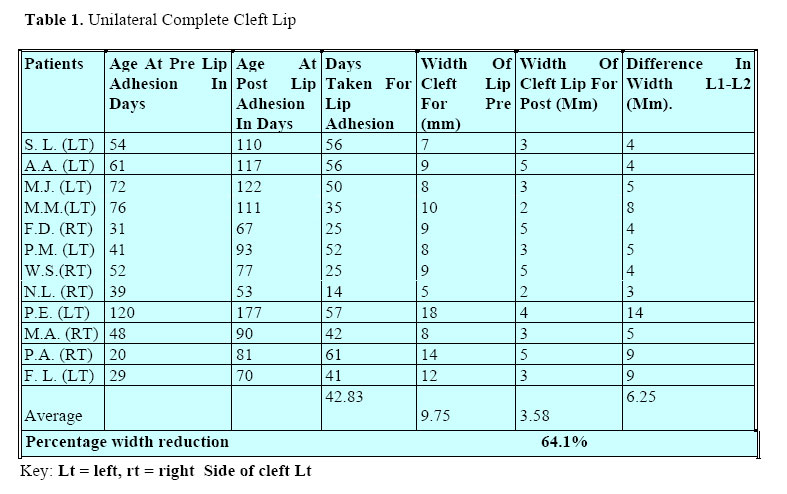
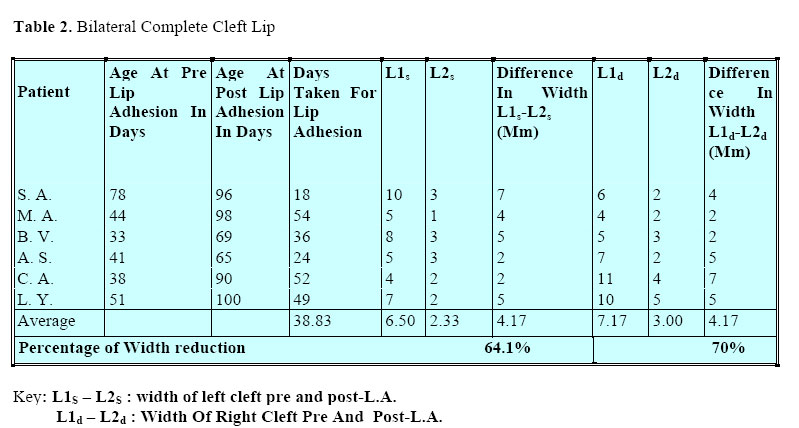
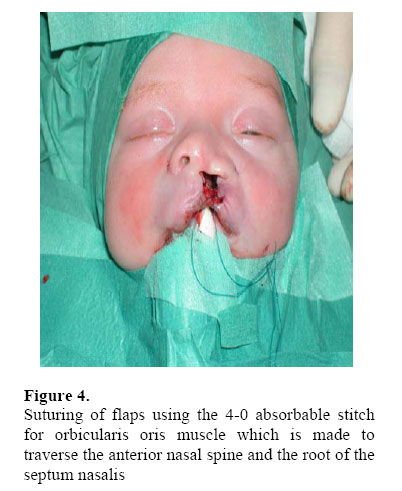
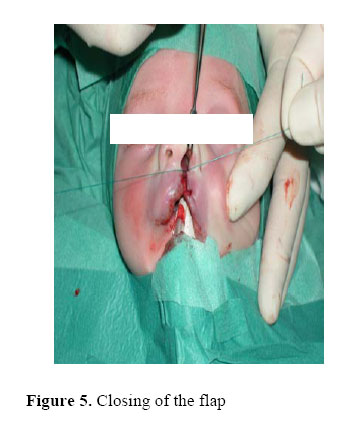
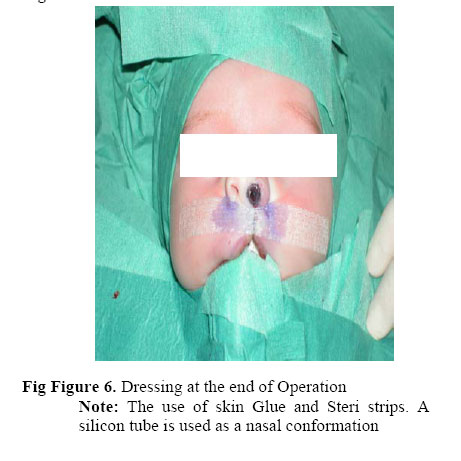
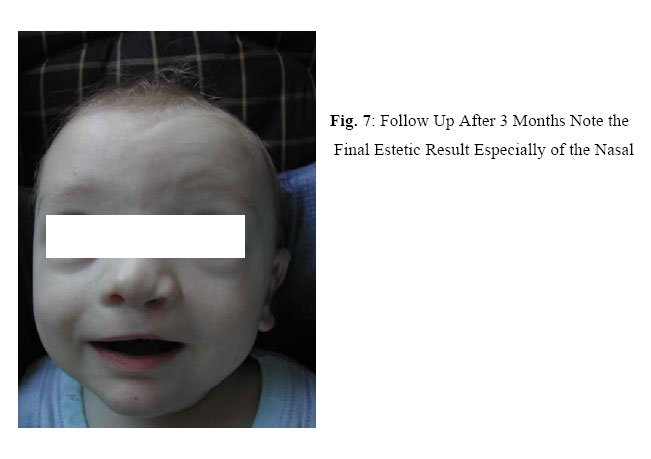
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 61-66 The Role of Lip Adhesion in the Treatment of Cleft Lips E.W Kalanzi1 FCS (ECSA), Gian luca Gatti2, Alessandro Massei3 1Plastic surgeon, Department of Surgery, Mulago Hospital, P.O Box 7051, Kampala, Uganda. Code Number: js04041 Background:Wide complete cleft lips, if repaired under tension result in a tight lip with inadequate lip elements, often with a thin vermilion and a whistle deformity. This is made worse by the inextensible, excessive scar tissue that results. In case of bilateral complete clefts, the problems are even more severe as seen by the dystrophic and dyschromic scar tissue. This combined by large alar bases and an almost absent columella make the picture very unaesthetic Though lip adhesion has been proved to diminish the cleft width, some authors have questioned its benefits as exaggerated and others like, George Scrimshaw, has called it “a passing fad”. This study was done to show the effectiveness of lip adhesion and to reassert its importance in the treatment of wide clefts. Introduction Lip adhesion (L.A) is a preliminary operative procedure that prepares a wide unilateral or bilateral cleft lip deformity for the definitive repair by converting the wide cleft into a much less difficult incomplete cleft. Various methods of decreasing a wide unilateral cleft or reshaping and positioning the protruding premaxillary segment in bilateral cleft have been described. These include: extra oral traction devices using for example head caps and elastic bands and intraoral orthodontic devices such as the Georgiade- Latham expansion appliance1 . These methods are complicated and expensive in that each has to be custom-made. They often require services of an expert neonatal orthodontist and the maximum cooperation of the child’s mother. In addition in case of the orthopedic plate, the child quickly develops a dislike to it and may lead to psychological trauma. L.A facilitates the treatment of wide clefts in the most gentle and natural way. In addition it has the following advantages: 1) molding of the alveolar segments, 2) improved nasal contour, 3) increased orbiculars oris tissue and, 4) increased vertical height of the lateral and medial lip elements. However L.A, though a good technique, has received a lot of criticism. Some authors have alleged that its benefits are exaggerated, others have expressed fears that it causes unestimatable damage to the growing maxilla, while still others such as Scrimshaw2 have called it “a passing fad” and that it is an unnecessary procedure which increases morbidity to an already "unfortunate” deformed child. While most of the questions raised by the critics have been answered in the past by various authors like: Randall3 , Skoog4 , Furnas5 , Hellquist6 , Semb7 and others, the purpose of this study is to present our experience with lip adhesion (L.A) at Cisanello Hospital, Pisa - Italy. Patients and Method Twenty-two patients were treated with lip adhesion in the period between May 2000 and May 2003 in the department of Plastic Surgery – Cisanello Hospital, Pisa, Italy. The indication for lip adhesion (LA), was considered a wide alveolar cleft (gap>7mm wide) with severely malpositioned maxillary segments in which primary cheiloplasty would have been complicated by this discrepancy. Severe protrusion of the premaxilla in bilateral clefts was another indication for L.A. Of the 22 patients treated, 7 patients had left unilateral complete cleft lip and palate, 5 patients had right unilateral complete cleft lip and palate, 8 patients had complete bilateral cleft lip and palate, 2 patients had bilateral cleft lip with one side complete and the other incomplete. Four patients were excluded from the study because of inadequate data. L.A was performed under general anaesthesia using Randall’s technique3 at an average age of 67 weeks, and the final cheiloplasty, by the technique of Tennison8, modified by Massei9 at an average age of 9 weeks. Closure of the palate was done at 5 months of age using the technique of Veau-Wardill-Nylen10-11 . In bilateral clefts the L.A was performed in one stage on both sides using Randall’s technique at an average age of 5 weeks. In case of bilateral cleft lip with one side incomplete, the L.A was done on the side with the complete cleft. Final cheiloplasty was done at an average age of 9 weeks using Mulliken’s technique12 . Photographs and impressions were taken prior to the operations. The impressions were made utilizing a special molding material (Alginoplast fast set-Heraeus-Kulzer dentists material). Immediately thereafter, casts in Plaster of Paris (Snow White Plaster No 2 of Kerr) were molded out of the impressions. At the time of the cheioloplasty, on average at 5-6 weeks, another set of impressions, photographs and casts was done. The width of the cleft was measured from the dental plaster models as the maximum distance between the alveolar segments. In the bilateral clefts, the maximum distance between the alveolar segments on both sides was measured. Results Tables 1 and 2 show that lip adhesion L.A, on average, achieved a reduction in the cleft width of 64.1% for unilateral complete clefts after 42.8 days. Whereas for bilateral clefts, L.A achieved a reduction of cleft width of 64.1% for left clefts and 70% for right sided clefts after an average of 38.8 days. DiscussionPreoperative positioning of the maxillary elements presents an improved platform for the closure of the clefts. The alignment allows dissection of the mucoperiosteum out of the cleft to create a tunnel across the bony gap into which bone can form and eventually teeth can erupt. This improves the functional and the esthetic result. L.A diminishes the cleft width, redirects the orbicularis oris fibres, gives a secure muscle and mucosal union and allows a simple and satisfactory final repair. The mechanism of action of L.A is thought to come from the orbicularis muscle, which during the procedure is brought into continuity across the cleft. It pulls the maxilla on the cleft side anteromedially as the patient laughs or cries; thus the forces that ordinarily would increase the deformity are now engaged in its reduction. The study showed that L.A, on average achieved a reduction in width of 64.1% for unilateral complete clefts after 42.8 days. This was in keeping with previous findings by Rintala and Haataja13, Randall and Graham14 and Pool and Farnworth15 except that their results were achieved after a longer period after L.A. It was found that the younger the patient is when L.A is done, the faster it takes for the maxillary segments to mold themselves13. For bilateral clefts, we achieved almost the same percentage of reduction of cleft width (64.1-70%) as in unilateral clefts, unlike previous authors who had achieved less effect with bilateral clefts. This could be explained by the younger age at L.A as the maxillary segments are better molded. The wider side of the cleft was found to be more moldable than the less severe side and in case where the cleft was symmetrical, L.A offered a lesser effect. Conclusion Lip adhesion is a simple technique that converts a complete wide cleft of the lip to an incomplete cleft in both unilateral and bilateral clefts. Although this adds an operative procedure to the usual lip repair, it makes the definitive closure simpler and easier. This results in improvement in the primary definitive repair with less need for secondary operations. Early lip adhesion should form an indispensable part of the cleft lip repair protocol References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04041t1.jpg] [js04041f1.jpg] [js04041f7.jpg] [js04041f5.jpg] [js04041t2.jpg] [js04041f2.jpg] [js04041f3.jpg] [js04041f4.jpg] [js04041f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}