 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 74-77 Femoral Hernia At Mulago Hospital, Uganda Odula P O. BSc (Anat), MMed (Surg), Kakande I. MMed (Surg), FCS (ECSA) Department of Surgery, Mulago Hospital. P.O. Box 7051, Kampala – Uganda. Code Number: js04044 Objective: To determine the incidence, pattern and the immediate outcome of femoral hernia surgery in Mulago Hospital. Introduction Femoral hernia is a variety of groin hernia. It usually presents as a defect in the fascia transversalis that is exploited by a peritoneal sac similar to the patent processus vaginalis in an indirect inguinal hernia exploiting the deep ring in the fascia transversalis of the posterior wall of the inguinal canal. Alternatively, similar to a direct inguinal hernia, the peritoneal sac of the femoral hernia may expand into an acquired defect of fascia transversalis in the femoral sheath to eventually herniate outside the canal. Therefore, femoral hernias can be classified into 5 groups as follows:
Femoral hernias are not as common as inguinal hernias. Femoral hernias account for about 1.2% to 10% of all groin hernias1,2. In British practice 50% of femoral hernias are admitted as emergencies with strangulation2. In Nigeria, in a 5-year study done at a teaching hospital, only 5 patients presented with femoral hernias out of a total of 111 groin hernias seen3. In a 14-year period Miller4, while working in different parts of Kenya, saw only 3 cases of femoral hernias. He further noted that by 1961, no operation for femoral hernia appeared on the operation lists at Kenyatta National Hospital in Nairobi4. In a review of intestinal obstruction at Mulago Hospital in the years 1958 to 1960, femoral hernias accounted for 12% of the strangulated hernias5. Whereas in Kampala, for every one man with a femoral hernia there are nine women6 the male to female ratio is 1.2 to 1 in the West African Hausa7. The aim of this study was to determine the incidence, pattern and immediate outcome of femoral hernia surgery in Mulago Hospital. Materials and Methods The study was conducted at Mulago National Referral and Teaching Hospital, which also serves as a Kampala district hospital. The study population consisted of 13 patients of all ages presented to the surgical wards and clinics with femoral hernias and subsequently underwent surgery over a one-year study period. Patients presenting for elective surgery with uncomplicated femoral hernias but had associated obstructive uropathy, chronic obstructive airways disease or chronic intestinal obstruction and those who refused to give consent were excluded from the study. After applying the exclusion criteria, the femoral hernia patients were assessed pre-operatively. Thereafter, each patient was followed up during surgery and during each post-operative weekday until the day of discharge. If the patient was discharged within a few days then, he or she was followed up in the surgical out patient clinic on the seventh post-operative day. During the follow up after surgery, post-operative complications were noted. In that aspect postoperative superficial wound infection was defined as:
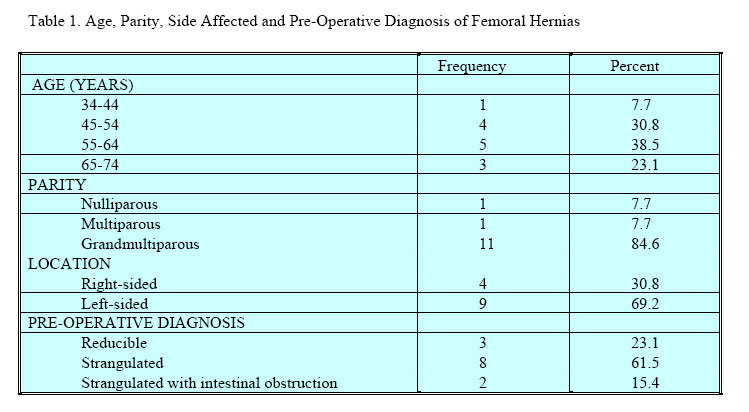
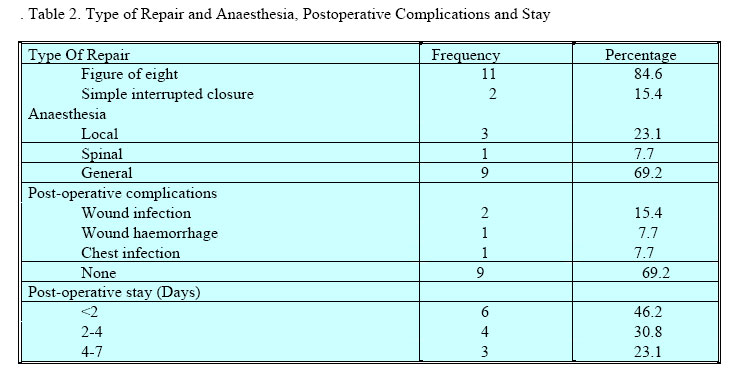
Results During the period under review, a total of 160 emergency and 48 elective groin hernia repairs were done. Of these, 13 were femoral hernias were operated on in 12 months. Ten (76.9%) presented as emergency and 3 were elective cases. Three (23.1%) were operated on electively. None was recurrent femoral hernia. All the patients with femoral hernias were females. The age distribution, parity, pre-operative diagnoses and location are shown in Table 1. The youngest patient with femoral hernia was 42 years old while the oldest was 70 years with a mean age of 54.6 years. Eleven patients were aged above 44 years. Four patients right-sided hernias while 9 (69.2%) had left sided femoral hernias. At surgery, no cases of gangrene were seen in all the 13 patients. A figure of eight stitch to the femoral canal was the most frequent repair (84.6%) performed for femoral hernias. The mean post-operative hospital stay was 2.4 days.The three patients who stayed longest had presented with strangulated hernias. (Table 2) Discussion This study has shown that femoral hernia represent 6.25% of emergency groin hernia surgery and similarly 6.25% of elective groin hernia surgery. Thus for every femoral hernia seen in this study there were 16 inguinal herniae. This study confirmed what Kingsnorth9 observed that femoral hernias are very rare under the age of 35 years and most common in multiparous women. He further suggested that femoral hernias were as prevalent in men as in nulliparous women. Only one patient in our series was nulliparous and no males were seen. The aetiology of femoral hernia is still ill understood. In contrast to inguinal hernia, there is no easy embryological explanation. The wider femoral canal in females due to their wider pelvis and/or the smaller size of the femoral vessels may explain why females are more predisposed to femoral hernias than males10. In tropical Africa, femoral hernias are rare compared with the Western world. It is postulated that the frequency of inguinal lymphadenitis due to chronic foot sepsis, resulting due to waling bare footed, which involves Cloquet’s node in the femoral canal may be protective in preventing femoral herniation in Africa11. Other authors have suggested that the smaller pelvis seen in African women compared to their European counterparts may explain the reason why the incidence of femoral herniation in Africa is much lower11. The apparent similarity in the distribution of onchocerciasis and femoral hernia in West Nile District of Uganda led to the filarial disease being considered as an aetiological factor in the causation of femoral hernia12. Weight loss in the old while the oldest was 70 years old whereas, the overall mean age was 54.6 years. Eleven patients 11(84.6%) were aged above 44 years. Four elderly female or a previous inguinal operation have also been associated with femoral herniation2,13. The fact that femoral hernias are most frequently found in middle-aged women suggests that intra-abdominal pressure and the stretching of aponeurotic tissue consequent on pregnancy are important factors that should not be ignored14. Repair of a femoral hernia follows the same canons of repair as an inguinal hernia repair. The peritoneal sac is isolated and excised, the fascia transversalis defect is repaired and then this repair is reinforced by adjusting the aponeurotic attachments. Three approaches to femoral herniorrhaphy are described and because none of these is universally applicable, the surgeon must acquaint himself with all the three. These are:
The crural approach is recommended for elective operations and to the occasional or novice surgeon. If a visceral strangulation is present it is best to perform a standard lower paramedical incision and deal with the crisis through an incision, which is familiar to most abdominal operators. With an emergency situation, or for the inexperienced surgeon, this is no place for an anatomical extravaganza. It is largely the efforts of Lichtenstein (Tension free hernioplasty), which have popularised the use of synthetic prosthetic mesh. Controversy still surrounds the ideal material. Polypropylene, Dacron, and expanded PTFE (polytetra fluoro ethylene) being some of the products currently in use. Excellent results of several thousand operations performed by the Lichtenstein technique using polypropylene mesh have been reported2,15. Plastic mesh can be applied as an onlay mesh or as a hernial margin cuff (selvage), which is then used as a buttress for conventional sutures. A more controversial use of prosthetic materials concerns its use configured as a swatch, bung, plug, or sutureless patch. In this context a roll or dart of material is placed in a hernial orifice with or without suture to obstruct the passage of the hernia to the exterior. A sutureless patch may then be placed over the whole of the posterior wall to reinforce this “swatch” 16. Since the pioneering work of Ger17, there has been an explosion of interest in laparoscopic hernia repair following closely on the heels of successful adoption of the laparoscopy for cholecystectomy. At this point in time, the laparoscopic operation is rapidly evolving and will require further study and better understanding of the anatomy. As techniques and technology improve, this operation may find its way into the general armamentarium of the hernia surgeon. Nevertheless, surgeons should not be pushed prematurely into mass utilization of this as yet unproven technique9. Wound haematomata formation can spell disaster for any hernia repair. Poor surgical technique resulting in tissue ischaemia combined with haematoma formation would ensure inhibition of local defences while providing the bacteria with a perfect milieu for division18. Compression of femoral vein can occur if sutures or prosthesis are placed too far laterally in femoral hernia repair. Oedema of the lower limb and pulmonary embolus could be the presenting signs of femoral vein compression. Once the diagnosis has been confirmed by phlebography, systemic anticoagulation and reoperation should be undertaken immediately. Femoral hernias are still a problem in Africa and which can easily be missed while operating on another hernia. Meticulous physical examination, early diagnosis and quick operative intervention will go a long way in reducing the morbidity associated with femoral hernia surgery. Acknowledgments We are grateful to the residents who operated on some of these patients. We acknowledge the contribution of those who assisted during the preparation of this manuscript. We are indebted to Alice Waswa, Department of Human Anatomy, Moi University for secretarial assistance. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04044t2.jpg] [js04044t1.jpg] |
| |||||||||

{kind=link}
{kind=link}