 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
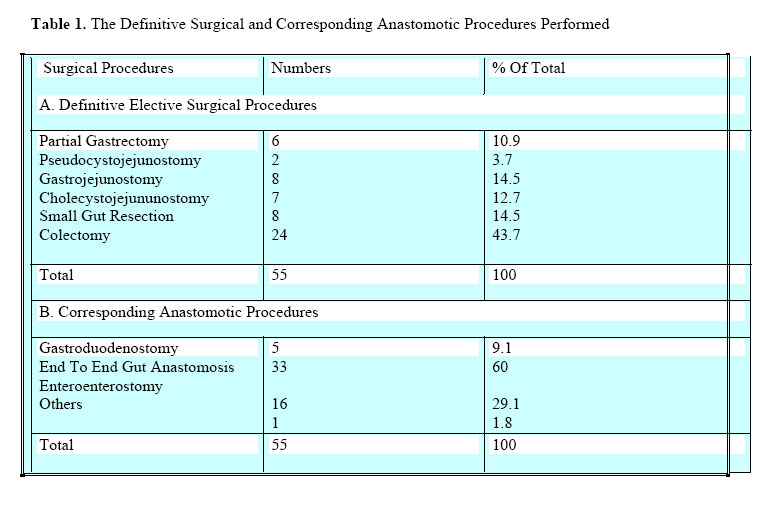
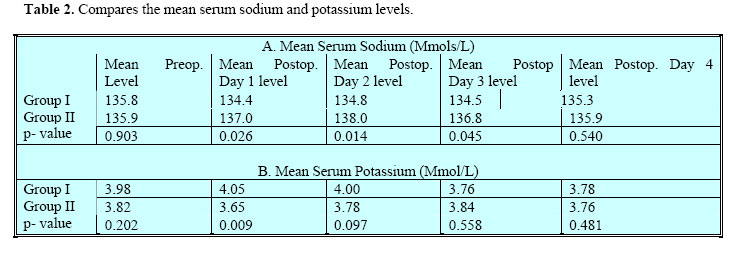
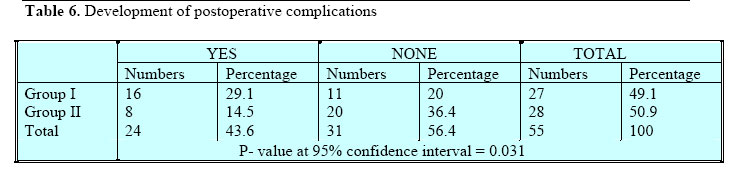
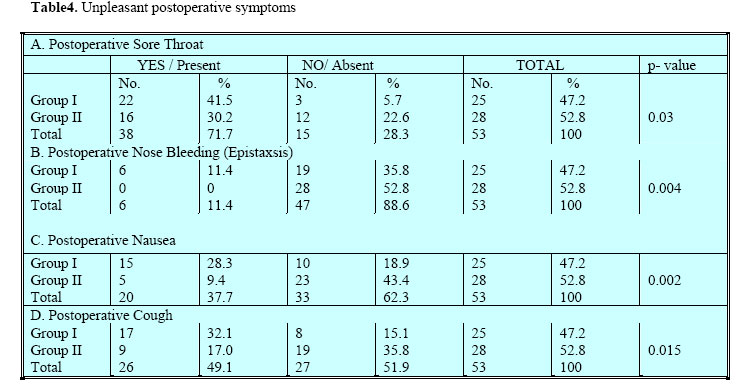
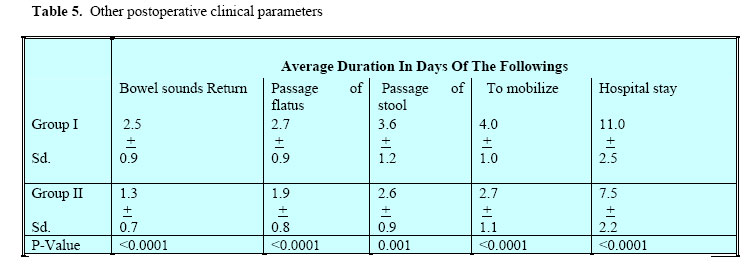
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 78-83 Routine versus Selective Postoperative Nasogastric Suction In Mulago Hospital.Ocen W MMed (Surg), Kakande I, FCS (ECSA), Sebbaale A, FCS (ECSA). Department of Surgery, Mulago Hospital, P.O.Box 7051, Kampala-Uganda. Code Number: js04045 Background: Nasogastric suction is a common routine postoperative procedure in abdominal surgery. Yet there is little scientific justification for it. This paper reports a comparision of routine with selective postoperative nasogastric tube suction in evaluating patients undergoing laparotomy. Introduction Since its inception by Levin in 1921 and popularisation by Wangensteen1 in 1933, Nasogastric suction has become one of the routine procedures in postoperative abdominal surgery2 and yet there is little scientific justification. With the advent of fast track and day care surgery in this modern era, the search for postoperative care protocols, which reduces costs, postoperative morbidity and shortens the duration of hospital stay continues to dominate surgical practice3 . Despite its importance in certain surgical abdominal conditions, various studies have shown that routine postoperative nasogastric suction is associated with higher rates of postoperative complications4,5,6,7,8,9,10,11,12 . These complications coupled with restrictions in mobility and the psychological discomfort has raised doubts about the benefits of routine intubation after elective gastrointestinal tract surgery13,14,15,16 . Currently, routine nasogastric suction as a prophylaxis against transient postoperative paralytic ileus is a common practice in Uganda despite the high labour demand required for its standard care. The purpose of our study was to compare the effects and outcomes of routine versus selective nasogastric tube suction following elective gastrointestinal tract surgery with respect to: serum electrolyte changes, postoperative complications, duration of return of bowel sounds and that of hospital stay. Patients and Methods Over a six month period, 55 general surgical patients from the three general surgical firms who underwent elective gastrointestinal tract surgery at Mulago hospital were prospectively randomised into group I and group II after a routine preoperative clinical assessment, preparation and baseline serum electrolytes. Patients in-group I had French 18 Ryles nasogastric tube inserted and connected to a drainage bag intra-operatively for drainage. Group II were not intubated unless they failed in the postoperative period. Failure in group II was defined by abdominal distension in excess of 10 cm coupled with absent bowel sounds. We excluded patients who had emergency surgery, children and infants; patients with impaired levels of consciousness and those who had repeat laparotomy. Baseline abdominal girths were obtained by measuring the abdominal circumference at the level of the umbilicus. Group I had intermittent eight hourly suction with a cone tipped 60mls syringe to remove any blockage in the tube that was left in situ till passage of flatus. The amount of NG aspirate in 24 hours in group I was measured and recorded. Postoperatively, patients were maintained on a combination of normal saline and 5% dextrose till they were able to take enough orally. Serum electrolytes in both groups were determined and recorded for four consecutive postoperative days. Patients were followed till discharge or stitch removal for other outcome variables like bowel sounds, postoperative complications and length of hospital stay. Data were analysed using Chi- Square and student t- test with a p-value of< 0.05 taken as being significant. Results Analysis was done for 55 patients, 27 (49.1%) of who were assigned to group I and 28(50.9%) to group II. There was a male to female ratio of 3:2 and a mean age of 45.3 years. Two diabetic patients out of the 28 patients (7.14%) in group II failed. A total of 55 different definitive surgical procedures with corresponding 55 anastomotic procedures were done on these patients (Table 1). The commonest definitive operations were colectomy (43.7%), gastrojejunostomy (14.5%) and small gut resection (14.5%) (Table 3). Group I had a lower mean serum Na+ level than those group II and this was statistically significant on day1, 2&3 with the respective p- values of 0.026, 0.015 and 0.048. Group II generally had a lower mean serum K+ than group I but this was only statistically significant on postoperative day1 with a p-value of 0.009 (Table 2). The mean nasogastric aspirate peaks on the 2nd postoperative day and there after decreases in the subsequent postoperative days. There were more symptoms of postoperative sore throats, postoperative epistaxisis, postoperative nausea and postoperative cough developed in group I than group II and these differences were statistically significant with respective p-values of 0.03, 0.004, 0.002 and 0.015 (Table 6). Group I took longer to: get bowel sounds, pass flatus & stool, mobilize and be discharged with the respective p-values at 95% confidence interval as shown in the Table 7. There were more minor postoperative complications developed in group I than group II and this difference was statistically significant with a p-value of 0.031 (Table 8). Discussion Although nasogastric suction has been regarded as a standard postoperative care since the 1930’s16, improvements in surgical techniques, anaesthesia and postoperative management has led many surgeons to question this belief. In this study, two patients in group I, both of whom had diabetes mellitus as a co-morbid condition failed representing a failure rate of 7.1%. Although diabetes mellitus may act as a factor to delay return of normal physiology of the gut in the postoperative period, further analysis did not show any statistical significance. Generally, the mean serum sodium in the two groups of patients was lower than figures quoted from the western world reflecting a similar finding by Kiyengo17. Group I had a lower mean serum sodium and a slightly higher mean serum potassium in the postoperative period compared to group II which were only statistically significant on day 1,2 &3 for sodium and day 1 for potassium. The postoperative serum sodium levels normalized on the 4th postoperative day whereas that of potassium remained fairly constant after the 1st postoperative day. A low mean serum sodium levels reflects its loss in the nasogastric aspirate, which however did not cause clinical hyponatriaemia. The normalization of serum Na+ levels on the 4th postoperative day coincides with the removal of the NGT and probably a reduction in the effects of surgical stress by this time. The significant difference in mean serum potassium levels in the two groups on the 1st postoperative day is probably due to postoperative stress response18. Soon after the 1st postoperative day, the body adjusts its physiology and jealously guards against any significant fluctuation in the serum level of potassium at the expense of other electrolytes like sodium and hydrogen ions19. This explains the insignificant difference in the serum level of potassium in the two groups after the 1st postoperative period. Majority of patients in group I developed unpleasant postoperative symptoms of sore throat, epistaxsis, nausea and cough on the 1st postoperative day which persisted for 4-5 days 4,5,10,13. The presence of a nasogastric tube has a mechanical effect of causing direct trauma to the nasopharyengoesophageal mucosa, stimulating the gag reflex and above all assisting in the translocation of microorganisms from the mouth, upper part of oesophagus and the pharynx into the respiratory tract and its eventual colonization20. The presence of NGT encourages mouth breathing with no air being filtered of particulate matters, which irritate the upper airways. Although there were more postoperative cases of vomiting in the NGT group than in the non NGT group, this difference was not statistically significant. Vomiting in the postoperative period does not only depend on the presence of NGT but on a number of many other postoperative factors like the drugs used, postoperative pain reflexes in the abdomen, infection amongst others. Out of the 25 patients of group I whose results were analysed, 15(60%) developed postoperative complications compared to 8(28.6%) in group II. This difference was statistically significant with a p-value of 0.031. These postoperative complications ranged from clinical chest infections to clinical laryngitis, overt wound sepsis, wound dehiscence and nasal septum necrosis. Postoperative clinical chest infection occurred soon after surgery but resolved faster in group II than in group I. There was however no serious postoperative complications like anastomotic leaks in the two groups. This finding is consistent with that of Bauer Joel etal.21 The higher cases of postoperative complications in group I could be attributed to the role of NGT in translocating microorganisms to the respiratory system, prolonging the duration of postoperative immobility with its associated untoward effects, decreasing protective airway reflexes with a higher risk of hypostatic pneumonias and above all, in delaying early enteral feeding which has been proven to stimulate the immune system and quicken postoperative healing6,22. There were more delays in the return of bowel sound, passage of flatus & stool and ambulation in group I than group II. The mean duration in days taken for the return of bowel sound was 2.5 days (60 hours) for group I and 1.3 days for group II. On average, group I took 11 days in the hospital compared to 8 days for group II. These differences were statistically significant (respective p-values < 0.0001). This finding agreed with that of Montgomery etal2 in 1996. A nasogastric tube keeps the pharyngeoesophageal junction open allowing air in during inspiration to cause more distention and, being a foreign material, NGT prolongs and increases the extent of post surgical inflammation and abdominal distention with subsequent increase in the duration of the transient post surgical paralytic ileus which delays the return of bowel activity23. It is probable that the presence of a NGT mechanically interferes with gut peristalsis subsequently resulting in a delay in return of bowel activity. The passage of flatus and stool is dependent on the bowel activity. A delay in return of bowel activity by the presence of a nasogastric tube in group I during the postoperative period automatically prolongs the duration taken to pass flatus and stool. Mobilization of the patient in the postoperative period is dependent on the presence of a NGT. The longer it is kept in place the longer will be the duration of patients’ restriction in bed. Prolonged immobilization after surgery infact enhances the risk of postoperative complication like DVT and delays recovery 21,24,25,26. All these effects of NGT therefore act indirectly to prolong the patients’ hospital stay. Conclusions We conclude that postoperative NGS significantly affects serum sodium levels, delays return of normal bowel activity and prolongs hospital stay. Routine NGS is associated with high incidences of postoperative complications. Our study was however unable to determine the type of surgical patients who should be intubated as a routine. We believe that selective postoperative NGS in elective abdominal surgery could help in reducing; postoperative morbidity, length of hospital stay and above all, hospital and national health expenditures. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04045t5.jpg] [js04045t6.jpg] [js04045t4.jpg] [js04045t2.jpg] [js04045t1.jpg] [js04045t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}