 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
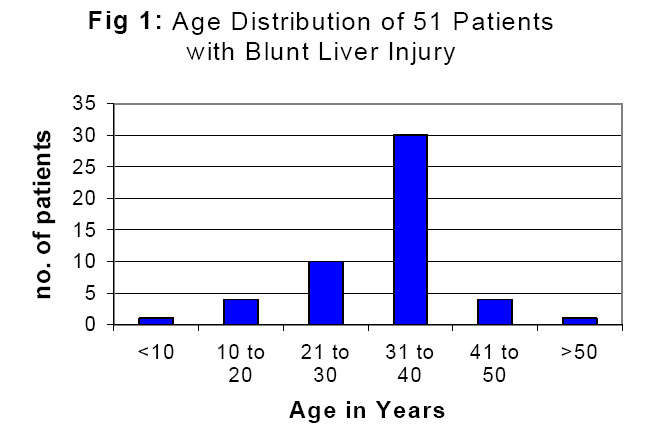
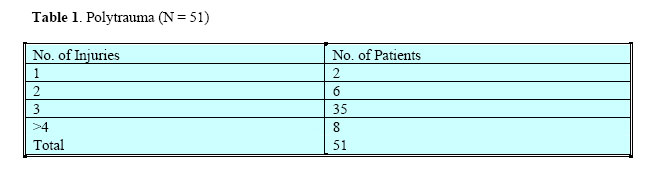
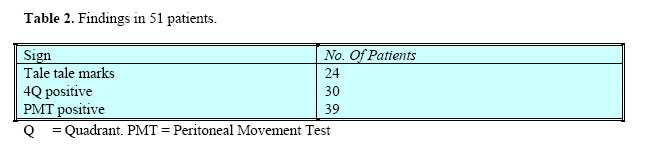
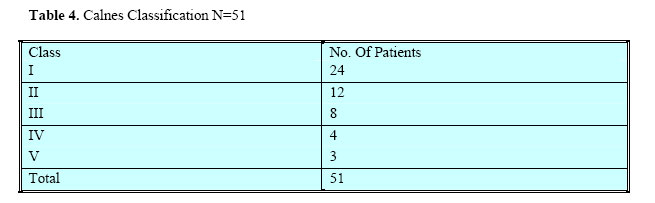
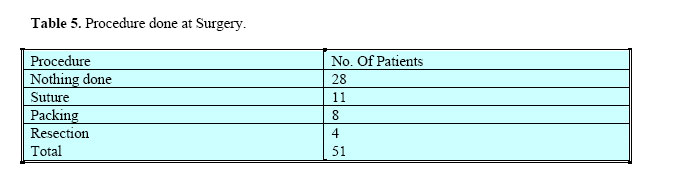
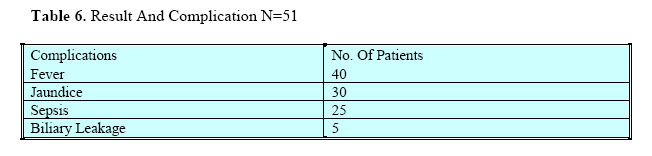
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 85-88 Blunt Liver Trauma In Mulago Hospital Gakwaya A M Senior Consultant Surgeon, Mulago hospital. P.O. Box 7051, Kampala, Uganda. E-mail: gakwaya@utlonline.co.ug Code Number: js04047Background: The paper presents 51 patients with blunt liver injury in Mulago national referral and teaching Hospital for Makerere University between Jan.1998-Jan.2003. Introduction Liver injury has been studied extensively in Europe and Asia1 . The commonest cause has been cited as Road Traffic Crash (RTC)1 . In 1982 Calne2 reported 26 cases and classified the liver injuries. Specific investigations for liver trauma include ultra sound and CT3. The patients who are haemodynamically stable are treated non-operatively and those who are unstable are treated operatively. The usual operation is laparotomy and then either do nothing, suture, pack, resect or transplantation4,5 .Liver surgery is associated with many postoperative complications of haemorrhage, sepsis6 and others. The mortality in developed countries is 5% for penetrating and 10% for blunt injuries1 . The main objective of this study was to determine the prevalence, causes, demography, clinical presentation and outcome of treatment of blunt liver trauma in Mulago Hospital. Patients and Methods This was a retrospective study of all patients who presented with liver injury at Mulago National Referral and Teaching Hospital between 1998 and 2003. All medical files which had diagnosis of liver injury were retrieved and the following data was collected: Age, sex, aetiology, number of injuries, symptoms, surgery done, post operative complication and mortality. Results During the period under review, a total of 51 patients were managed for liver injuries. Figure 1 shows their age distribution. The peak was between 31 - 40 years. The male to female ratio was 16:1. The cause in thirty out of 51 patients was road traffic crash followed by falls from a height (Fig 2). Forty-three patients out of 51 had 3 or more injuries. The commonest associated injuries were those of lower limb fracture (Table1). On admission, 20 patients presented with haemorrhagic shock. In 39 patients, the Peritoneal Movement Test (PMT) was positive (Table 2). All patients had a laparotomy. In the majority of patients a right upper paramedian incision was used (Table 3). Using Calne's classification of the liver injuries, 24 patients had class I (Table 4). In 28 patients, nothing was done at laparotomy (Table 5). Postoperatively, 40 patients had fever. There were 10 deaths (Table 6). According to Calne's classification there were 4 deaths in class II, 3 in class IV and 2 in class V (Table 7). Discussion This study has confirmed that like in other studies from elsewhere, Road Traffic Crushes are the major cause of liver injury and also the commonest cause of all other injuries7. The peak age of 31-40 years found in our series was in agreement with that found by Alison et al in 19911. The reason is because this age group is closely associated with RTC. The male to female ratio in this study is 17:1 is comparable with that reported by Pachet and other workers7. This is expected since males are normally more involved in many hazardous activities. The clinical features in liver trauma are vague and non-specific. However there are tale-tell marks such as were present in 30 of our patients. Although peritoneal lavage was not done in the present series, Schweizer8 showed that it is positive in 95% of liver injuries. A test that has not been descrided before in literature, “the peritoneal movement test (PMT)” was positive in 39 patients out of 51.The test is positive in the majority of patients with closed abdominal injury. A conscious patient is asked to distend his abdomen and then to relax it. The test is positive if the patient fails to go through the exercise because of pain, which indicates peritoneal irritation. However the test is nonspecific and does not indicate the point to the organ that is injured. Patients with liver injury may be haemodynamically unstable and may present in haemorrhagic shock requiring urgent resuscitation8 as was the case in 20 of our patients. Often the patients have polytrauma8. Thirty patients had at least 3 other injuries. Pachet et al7 found that 60% of liver trauma patients had other injuries Investigations In this study ultrasound and CT were not done. This was unfortunate since other studies1 have shown that when done, these investigations the number of patients treated non-operatively increases. Treatment In the present series, all patients underwent laparotomy. This was due to lack of modern technology in accident and emergency unit in our hospital. Otherwise the concept now is to treat the haemodynamically stable patient nonoperatively3,7.8. Hospitals that lack modern technology tend to do more laparotomies and have to face their associated complications and expenses. In this study the most commonly used incisions were the right upper paramedian, the hockey stick and in three patients, the abdominal thoracic. Currently, the left or right subcostal incision is considered the best incision8. It gives good access to the liver. The finding in this study based on Calne's classification were comparable to those reported by Schweizer et al8. Majority of the patients had Class I and II injuries. This may explain why in 30 (58,8%) of the patients nothing was done at laparotomy. The surgeons found that the liver has stopped bleeding. These are the patients (Calne's II & I) who would have most likely been managed nonoperatively had CT been available. Procedures acceptable in managing liver trauma include packing5,7,9. It allows control of haemorrhage and if need be referral to a referral hospital. At least two abdominal mops should be used, one posteriorly and the second anteriorly. The abdomen closed and reopened within18-24 hours. If there is delay in reopening the abdomen5 there are complications associated with the park e.g. high risk of infection6. The commonest complications seen after surgery were fever and jaundice. The Mortality rate was 20%. Death was related to both the grade of the liver injury and the multiplicity of the associated injuries. The 4 patients who died in class II had chest and head injuries. Conclusion and Recommendations U/S and CTS were not used routinely in Accident and Emergency unit in Mulago Hospital. Consequently unnecessary laparotomies were done. The mortality of 20% is high when compared to the 4-10% reported from elsewhere. It is recommended that:
References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04047t3.jpg] [js04047t4.jpg] [js04047t7.jpg] [js04047t6.jpg] [js04047t5.jpg] [js04047t1.jpg] [js04047f1.jpg] [js04047t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}