 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
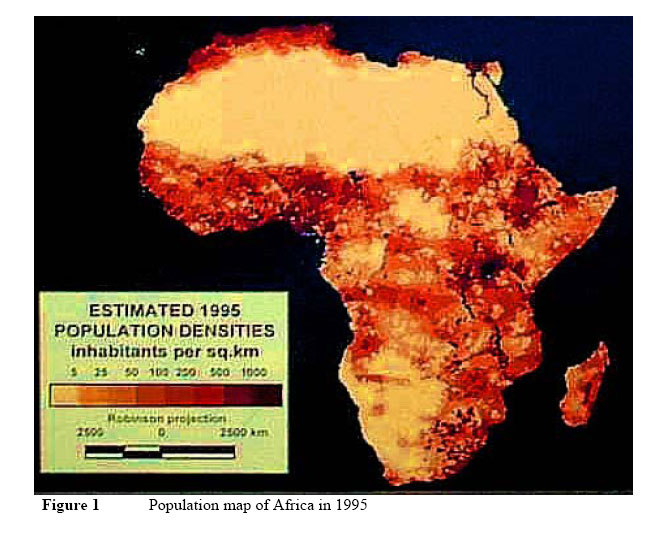
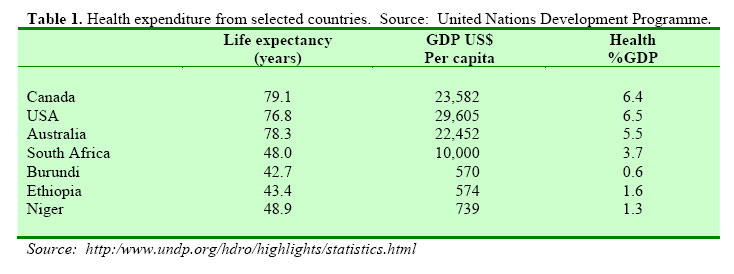
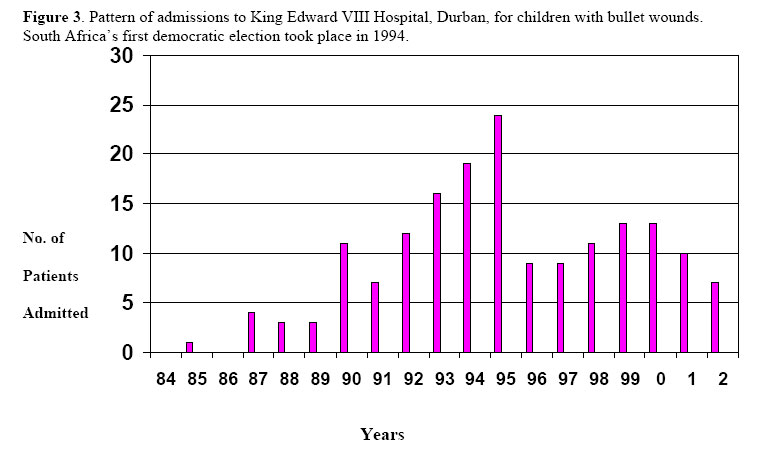
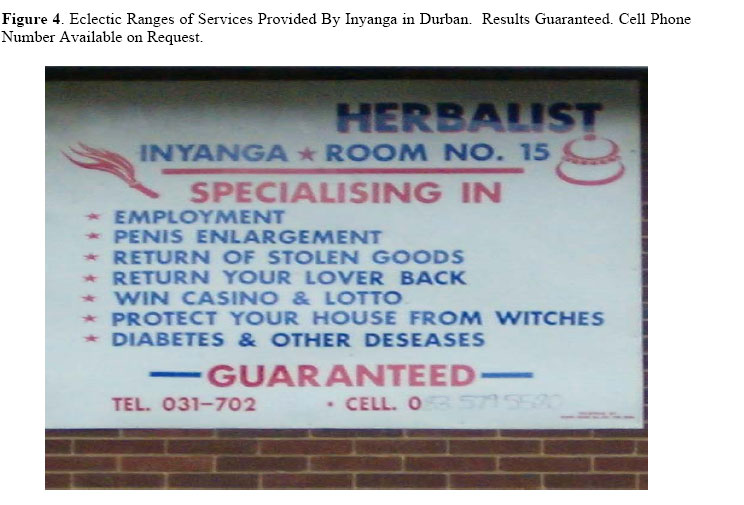
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 103-109 The Rahima Dawood Oration delivered in Harare, Zimbabwe on 2nd December 2004: The Paediatric Surgeon in Africa: Luxury or necessity Prof G.P. (Larry) Hadley, MB, ChB, FRCSEd Department of Paediatric Surgery, Nelson R Mandela School of Medicine University of KwaZulu-Natal, Private Bag 7, Congella 4013 Durban, South Africa. Facsimile:+27 31 2401667, e-mail: hadley@ukzn.ac.za Code Number: js04050 Being elected as the Rahima Dawood Traveling Fellow for 2004 has been a great honour and privilege. It has also been great fun and an enhancing experience. I am proud to have been the first surgeon from south of the Limpopo to be so honoured and to be only the second Paediatric Surgeon elected to this Fellowship. I am indebted to the Council of the Association of Surgeons of East Africa, the College of Surgeons of Edinburgh, and the Rahima Dawood Trustees for giving me this opportunity to visit colleagues and friends throughout the region. To witness their achievements in a resource-constrained environment has been humbling. I am, of course, equally indebted to colleagues in Malawi, Kenya, Uganda, Zambia and Zimbabwe who, without exception, made me feel welcome and who took time and trouble to share their experience with me. “Standing on the shoulders of a giant the dwarf can see further than the giant himself.” Pliny the Elder Were each generation of mankind required to invent the wheel we could never have developed the motor-car and each of us recognizes in his own career giants who have allowed us dwarves to stand on their shoulders and make what we can of the view. In my own career there are three true giants to whom I owe a huge debt. First is Mr. Dharam Nirmul, a South African general surgeon who now works in America. If I have any surgical skill at all it is due to his tutelage. He is a master of clinical diagnosis, patient care and of surgical technique, emphasizing gentle tissue handling and dissection. He was a very patient and generous tutor. Secondly Professor Lynne Baker, Head of Surgery at the University of Natal during my training who allowed me to develop an interest in Paediatric Surgery and who encouraged an academic approach to surgical practice. Thirdly my predecessor as Head of Paediatric Surgery at the University of Natal, Professor Robert E. Mickel who is infinitely experienced in the surgery of children and who taught me the importance of caring about, as well as caring for, our patients. “The one real object of education is to leave a man in the condition of continually asking questions” Bishop Creighton To these three individuals, and many others, I am grateful for a surgical education that recognizes the importance of asking questions, that is the basis of surgical research, itself a cornerstone of good surgical practice. What is a Paediatric Surgeon? To return to the topic of this talk, a Paediatric Surgeon can be defined as one whose practice is largely or wholly concerned with the diagnosis and management of the diseases and disorders of childhood and who has received special training in the management of these diseases and disorders. It is important to note that in terms of this definition a Paediatric Surgeon’s practice need not be exclusively paediatric, you may choose to call such an individual a General Surgeon with a Paediatric interest, or indeed whatever you wish, but the individual will have received special training in the surgical diseases of childhood. Paediatric Surgeons require special skills and attitudes because children are not small adults in any anatomical, physiological, pathological or psychological sense. They suffer from diseases and disorders unique to childhood with no equivalents in the adult population. Many adult surgeons find the paediatric patient, and especially the neonatal patient, an intimidating prospect. This does not necessarily work to the patients’ advantage. C.J. Barrington-Ward famously stated that “to treat an adult as a child is no misdemeanor, but to treat a child as an adult most often ends in disaster.” It is the recognition of this truth that justifies Paediatric Surgery as a discipline apart from adult surgery. Ex-Africa The map of Africa (Figure 1) shows an uneven distribution of the population with large areas of the Sahara and Kalahari deserts being virtually uninhabited whilst there are large concentrations of people along the eastern seaboard of South Africa, around the Great Lakes region in east Africa, and in Nigeria and other areas of West Africa. According to estimates from the United Nations Population Division in 20021, estimates that take full account of the HIV/AIDS pandemic and the difficulties that Africa has in feeding itself, the population of the continent will increase 2.5 times, or by nearly 1000 million people by 2050 that is in 45 years time. Interestingly the population of Europe will fall by nearly 100 million in the same time period. Thus in Europe we have an ageing population with a falling birth rate and in Africa the exact opposite. Within Africa, the populations of South Africa, Botswana, Lesotho and Swaziland will fall, largely due to disease, but this will be more than compensated for by the quadrupling of the population in countries such as Uganda. Ignoring this huge demographic shift will not make it go away!! It must also be remembered that the 1000,000,000 new people in Africa are all going to be children to begin with. Childhood is measured out by sounds and smells before the dark of reason grows.” Sir John Betjeman; Summoned by Bells lV. As clinicians concerned with the welfare of children it is our responsibility to ensure that our charges are able to enjoy that normal period of growth and development that we call childhood. Such enjoyment is not a privilege, it is a right. In sick children this normal process is disrupted. We must also recognize that sick children disrupt family dynamics and place exceptional strains on social and other structures. Both mothers and fathers are exposed to these stresses that may require specific attention from health care professionals. Paediatric Surgeons: Population One index of how ready we are to meet these challenges of the immediate future is the number of Paediatric Surgeons, already trained and practicing, relative to the population. In Europe there is approximately one Paediatric Surgeon for every 50,000 population. In South Africa, extrapolating from the data provided by Driller et al.,2 there is a Paediatric Surgeon for every 2,669,00 people, and South Africa is probably better endowed in this regard than many of the countries that neighbour it. These figures however mask the fact that in a European population most of the members will be adults; in Africa well over 50% of the people are children. Thus the paradox of a high number of Paediatric Surgeons for an ageing population with a low birth rate in Europe and the scarce resources of Africa. It may be more realistic to look at the number of Paediatric Surgeons per live births per year. In Austria there are somewhat less than 500 live births per paediatric surgeon, in the UK a little over 6,000. In South Africa there are 35,714 live births per paediatric surgeon. Thus if a pathology, such as oesophageal atresia, occurring once in every 3,000 live births is considered, the paediatric surgeon in Austria will have to wait 6 years to see the condition. This is hardly frequent enough to maintain operative skills let alone the skills of the care team. In contrast the South African paediatric surgeon will see approximately one every month. By extension of this argument it is clear that in Africa there is no imminent possibility of every child who needs surgery having that surgery performed by a specialist paediatric surgeon. The general surgeon is still going to have a considerable clinical exposure to children and childhood diseases. For this the general surgeon will need specific training. Paediatric surgeons do not intend to create a monopoly, merely to set the standards for the surgical care of children, to teach and to research. We have shown that it is possible to alter perceptions and responses of medical officers and surgical trainees in a relatively short period of time, but training in paediatric surgery is about education not teaching.3 “Education is what survives when what has been learned has been forgotten.” BF Skinner Africa is short of some 100 medical schools required to bring it in line with northern hemisphere norms. This relative paucity of training establishments is reflected in the inadequate numbers of doctors available to provide services to the community. The existing medical schools simply cannot keep up with the demand for medical personnel. Exporting medical students for training abroad often results in young doctors with inappropriate skills and knowledge who are out of touch with the needs and aspirations of the communities whom they are ultimately intended to serve. South Africa is well off relative to its neighbours in terms of medical schools but still well behind countries such as America and Egypt and still finds it necessary to send students abroad for training. The problem is exacerbated by the loss of trained medical and nursing personnel to developed countries that could well afford to train their own professionals but for whom it is economically advantageous to poach trained staff from the Third World. “The economic imperative” So-called First World countries spend between 5 and 6% of their Gross Domestic Product (GDP) on health care, translating into a cash expenditure of between $1,000 and $2,000 per head of population per annum (Figure 2)4. South Africa is able to spend 3.7% of GDP on health, translating into $370.00 per head. However it will be clear that even were a country like Burundi to increase its proportion of GDP spent on health to a level such as the 6.5% GDP spent in America, i.e. a ten fold increase, it would still only have available $30.00 per head of population for health care. So the limited health care resources are not simply a problem of uneven distribution within national budgets, they reflect the real poverty of the region, a poverty sustained by the neocolonial economic policies of so-called “developed” nations. But health care must acknowledge the economic imperative. “There is no finer investment for any community than putting milk into babies” Winston S Churchill 1943 This being so, primary health care has quite properly been the emphasis of caring governments throughout the region. It should be realized that the primary health care of many paediatric problems is immediate simple surgery. Cost-effective health care must also acknowledge the economic disaster of the HIV/AIDS pandemic. This is an African problem. The numbers of affected individuals in other regions are trivial compared to the disaster in sub-Saharan Africa. In our own region, KwaZulu-Natal 36.5% of the women attending antenatal clinics in 2002 were HIV positive with 18.4$ of the total population living with the disease5. One in eight of our health workers is HIV positive. The impact of these data will be devastating. It is going to be difficult to maintain a health service when 12.5% of the health care workers can no longer work There are similar crises looming in all professions from teaching, nursing, military personnel, etc. There are also important implications for the sustainability of South Africa’s economic development with an ailing workforce. A side effect of the pandemic that is already upon us is the rising number of AIDS orphans, not necessarily HIV positive themselves, who are being raised in dysfunctional groupings without the stability of parental care. There have been extensive internecine debates in our region about the funding and practicalities of providing HIV treatment to rural and informal settlement populations, but it now appears that the “rollout” is underway. (Table 1) “In the final analysis, it is our concept of death that decides our answers to all the questions that life puts to us.” Dag Hammarskjold, 1958 In the face of these financial and other constraints we, like many other countries, have evolved a sequential system whereby a patient percolates up to an appropriate level of care from the Base Hospital or Clinic, through the Regional Hospital where there is a General Surgeon, to the Tertiary Hospital with a Paediatric Surgeon available. Like any chain this is only as strong as the weakest link. In our practice the weakest links are triage or stratification, communication and transportation. To help alleviate some of these difficulties our region has invested quite heavily in Telemedicine or TeleHealth. Generally however we have learned that technology in Africa is unreliable, even though donors love it because it provides a surface for the application of a plaque. We have learned to accept all the help that we need, not all the help that is offered, and have come to realize the benefits of low-tech equipment particularly in transportation6. Our system of referrals recognizes our philosophy that Paediatric Surgery is a team event. For success to be achieved the primary care team must timorously make a diagnosis, our transportation team must safely effect a transfer to an appropriate level facility, our pre-operative preparation must be adequate, our anaesthetic and intra-operative skills must be of a high standard and our postoperative care, either in the intensive care unit or ward environment, and our follow-up of the patient must be effective. It is acknowledged that each member of the team has his own unique function, but we stand or fall together as a team. There is little point in performing surgery quite brilliantly if the post-operative care is inadequate and the patient succumbs to misadventure in the intensive care unit. One member of the health care team that is frequently forgotten is the community. If we do not mobilize the community to identify our health care priorities, failure is inevitable. In our communities in South Africa a worrying trend has been the incidence of gunshot injuries in children7. Our children are growing up in an environment where the possession and usage of a gun is equated to power and status. It has been estimated that there is a gun for every twenty people in continental Africa, most being the residuum of the wars that have plagued the continent, and continue to plague the continent. The children of our region paid a high price for freedom, and they continued to pay into the new dispensation as political disagreements between adults were(Figure 3). These were not the teenage gang reflected in childhood injuries members perpetuating a cycle of violence that dominate American experience with gunshot injuries in childhood. The mean age of our patients was 5 years. These were simply children who were in the wrong place at the wrong time surrounded by adults who should have known better. It is particularly distressing that for every patient that was admitted to the hospital with a gunshot injury, four were taken directly to the mortuary. Amongst the 20% that survived to be taken to hospital, this low percentage reflecting the poor emergency care services available in rural and informal housing areas as well as the size of the victims and the severity of even a low velocity bullet wound in a small child, 10% died and a further 10% were left with a life-long serious disability such as paraplegia, amputation or loss of sight. All had their potential reduced by their experience. Our children have paid a high price indeed. The solution to this sort of problem lies with the community. Children must be educated about guns and know of their dangers. Gun ownership should be seen as a sign of weakness not strength. The awful events in northern Uganda, in Liberia and in Sierra Leone where children became forced recruits into the military, must be denounced by us all in unison. When the community joins the teams there are no limits to what can be achieved. It is also important to get the traditional healers on-side. The inadequacy of our primary health care facilities is clearly demonstrated by the fact that 80% of our patients have consulted with the traditional healer before accessing formal medical structures8. When traditional healers act in a fashion complementary to medical practice their contribution can be enormous. However many still advertise impossible services, such as winning at the casino or curing HIV/AIDS and threaten the credibility of the entire profession (Figure 4). The Nelson Mandela School of Medicine has taken the initiative and signed a Memorandum of Understanding with indigenous healers in KwaZulu-Natal on collaboration in the health care system. This will, it is hoped, impact greatly on the practice of paediatric surgery in this region. One aspect of traditional care that is not helpful is the delay in presentation to hospitals of children with pathology that requires urgent treatment. A particular example is the child with a malignant solid tumour, most of which, if treated early, are compatible with long-term survival. However in Africa we are faced with the “Third World Triad” of advanced disease, significant co-morbidity and an inability of our patients to comply with treatment protocols that were derived and designed for use in First World countries. The most significant comorbidity that we see is sub-optimal nutrition that has a direct impact on outcome9. The solution to this surgical problem is not surgical. Thus there are challenges for all surgeons working in Africa. The advent of 1,000,000,000 more children, in addition to the large numbers of children currently being born, in a relatively small time frame means that the general surgeon will be unable to hide from children and childhood disorders. He is going to need training to learn appropriate ways of dealing with these patients. There is also going to be an increasing need for trainers, surgeons who devote much, if not all, of their time to the care of children. Now is the time to start training them, not as a luxury but as an urgent necessity. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04050t1.jpg] [js04050f3.jpg] [js04050f1.jpg] [js04050f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}