 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 9, No. 2, Dec, 2004, pp. 111-116 The Triple Assessment In The Pre-Operative Evaluation Of Patients With Breast Cancer In Mulago Hospital, Kampala – Uganda. Mande N1 , Gakwaya A M2, Byanyima R K3, Othieno E4. 1Senior House Officer, 2Senior Consultant Department of Surgery, 3Consultant, Department of Radiology, 4Consultant, Department of Pathology, Mulago Hospital, Kampala, Uganda Code Number: js04052 Background: Triple assessment has been recommended in diagnosis of Breast cancer in Uganda. This review analyses its diagnostic value in patients presenting with clinically malignant breast lumps. Introduction In UK and USA, the incidence of Breast cancer is 80-100:100,000. In Africa, the incidence is reported as 13-16 per 100,000 women3 . In Uganda, the incidence has doubled from 11:100,000 in 1961 to 22:100,000 in 1995 and has become third commonest malignancy, after cancer of the cervix and Kaposi’s sarcoma4,5. In 2003, Mulago Hospital, breast clinic registered 670 new patients; 15-20% of them had malignancy6,7 . More than 75% of the patients with breast cancer present late6 . The Breast Cancer Guidelines for Uganda recommends diagnosis of breast lumps by a triple assessment using minimally invasive procedures before definitive treatment8 . At the breast clinic in Mulago Hospital, the patients undergo routine clinical evaluation and are investigated by mammography and fine needle aspiration cytology (FNAC) in the triple assessment. Open biopsy is still in common practice as a diagnostic procedure, but it is invasive and risks escalating spread of malignancy. Mammography and FNAC though not conclusive, have been evaluated locally and the findings are valid and reliable9,10 . The triple assessment has been routinely practiced in the developed world since its earliest evaluation11,12 . The validity and reliability of the triple assessment in Uganda is not known, as no local studies have been done. Locally generated information is necessary to strengthen the national guidelines and influence health service planning to increase availability and access to the diagnostic facilities. The aim of this study was to determine the validity and reliability of the triple assessment in the pre-operative evaluation of patients with breast cancer in Mulago Hospital. Specifically the objectives were to evaluate the diagnostic outcome of clinical assessment, mammography and FNAC in isolation and when combined, using histology as the gold standard. Patients and Methods A cross-sectional study was undertaken in Mulago Hospital between January 2003 and April 2004. The Study Population was comprised of the new patients attending the breast clinic and those admitted in the general surgical wards with breast lesions clinically suspected to cancerous. All patients aged 18 years and above who presented with suspected breast cancer consented to participate in the study were included in the study. Patients with recurrent breast cancer on the same side and those with ulcerated breast masses difficult to compress at mammography, were excluded. Using the method of fixed numbers13,14 200 consecutive patients were recruited. All the patients underwent clinical evaluation, mammography and FNAC. Histology was done to confirm the diagnoses. Ethical considerations included seeking of permission to carry out the study from appropriate authorities and confidentiality All the subjects were interviewed and examined by the Principal Investigator who also did the FNAB. Clinical evaluation included the patients’ demographic details, history of breast disease and physical examination. Physical findings suggestive of breast cancer were hard irregular lumps, nipple elevation and retraction, areola thickening, peau d’orange, skin tethering and erythema, axillary lymphadenopathy. Regular mobile masses were considered benign. At mammography standard cranio-caudal and oblique views were taken. The radiologist’s findings and report were recorded as the radiological diagnosis. FNAB was taken from the lesion following aseptic procedure using 23G needle and 5ml syringe. Two slides of thin films were made and stained with a standard haematoxylin and eosin. The pathologist’s report was recorded as the cytological diagnosis. The clinical, mammography and FNAC diagnoses were respectively coded as:
Biopsies were taken from specimens removed after therapeutic surgery, diagnostic surgery or core needle biopsy in case of patients who declined surgery or those with inoperable disease. The histological report was coded as:
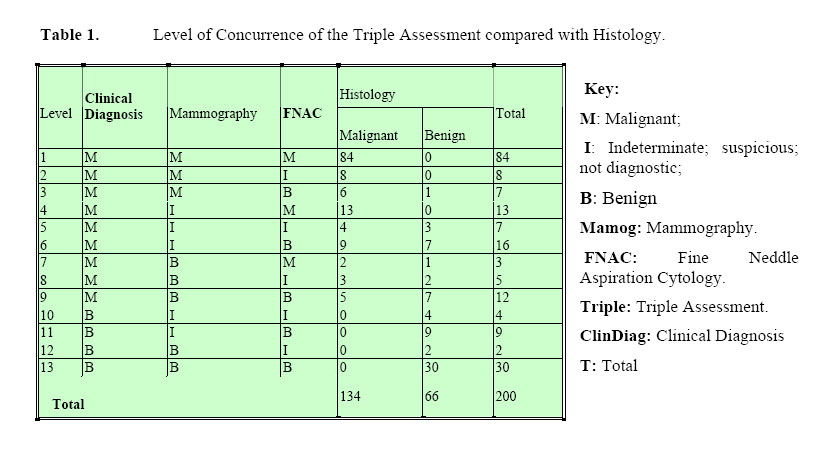
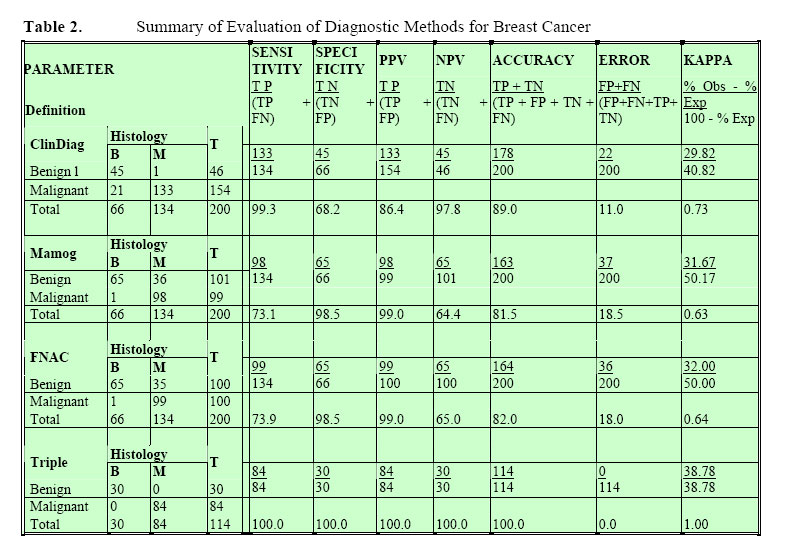
Definitive treatment was started when the three diagnostic procedures concurred. In cases of diagnostic discrepancy, a core biopsy was obtained from large tumours and wide excision biopsy done for small tumours of up to 3cm in size. Histology guided the subsequent modifications in treatment. Data was collected by a pre-tested questionnaire, coded and entered in SPSS version 10.0 statistical software for analysis. Variables were crosstabulated against histology, the gold standard. The sensitivity, specificity, accuracy, Positive Predictive Value (PPV) and Negative Predictive Value (NPV), accuracy and error were determined for the individual methods and when combined15,16. A p-value obtained for each observation was considered significant if found less than 0.05. The Kappa statistic was calculated for individual methods and their combination. A value above 0.75 suggested excellent agreement with histology, 0.40 to 0.75 was intermediate to good agreement and below 0.40 suggested poor agreement13,17. Results Out of the 200 patients recruited in the study, 194 (97.0%) were female and 6 were males. Their ages ranged from 19 to 88 with a mean of 48.0 years (p-value = 0.017). A third of the patients (33%) had histologically benign disease. Histology confirmed a diagnosis of breast cancer in 134 (67%) of the cases. Among them 131 (97.8%) were females. Three breast cancer patients were males; giving a female to male ratio of approximately 44:1 among those found to have breast cancer (p-value = 0.369). On examination, 71.5% of the patients were in good general condition – Kanorfsky scale above 70% (p-value = 0.000). Clinically, 154 patients were diagnosed malignant of who 133 was True Positive. Forty-five of the 46 diagnosed have benign lesions were True Negative (p-value = 0.000). The Sensitivity and specificity of Clinical examination was 99.3% and 68.2% respectively. The Positive Predictive Value was 86.4%. The Error was 11.0% and Kappa statistic 0.73. From mammography, 98 patients out 99 were True Positive. 65 patients out of 101 were True Negative (p-value = 0.000). The Sensitivity was 73.1% and Specificity 98.5%. The Positive Predictive Value was 99.0%. Error was 18.5% and Kappa statistic 0.63. From FNAC, 99 out of 100 patients were True Positive. 65 patients out of 100 were True Negative (p-value = 0.000). The Sensitivity was 73.9%, Specificity 98.5% and Positive Predictive Value was 99.0%. Error was 18.0% and the Kappa statistic 0.64.In the triple assessment, 84 and 30 patients were respectively confirmed by histology to have malignancy and benign disease (p-value = 0.000). The Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value and Accuracy were respectively 100.0%. Error was 0.0%. The Kappa statistic for the combination was 1.0. Table 1 shows the level of agreement of the diagnostic tests and Table 2 shows the findings of the tests compared with histology. DiscussionThe registration showed evidence of rising numbers of new patients at the breast clinic. On average, 2 new patients were diagnosed with breast cancer per week. Clinical evaluation of the patients showed high sensitivity (99.3%), and relatively moderate specificity (68.2%) and high error (11.0%). There was good agreement with histology (κ = 0.73). False positive diagnoses resulted from the high index of suspicion and prudence towards breast lumps. False negative clinical diagnoses arose from atypical presentations commonly seen among patients below 30 years. Diagnosis of breast cancer was straightforward with advanced disease. The findings were compatible with findings of other studies10, 18, 19, 20, 21, 22,23 . On mammography there was moderate sensitivity (73.1%), high specificity (98.5%), high PPV (99.0%) and high error (18.5%). There was moderate agreement with histology (κ=0.64). A variety of radiological patterns were seen at mammography. Definitive diagnoses were made from hard lumps, which produced stellate, or spiculated appearances. False negative or indeterminate diagnoses were from soft, cystic or ill-defined lumps, and lumps close to chest wall. With improved technology and experience a high specificity is expected from mammography. These observations are consistent with findings in local and international studies7,10,16-21, 24,-27 FNAC showed moderate sensitivity (73.9%), high specificity (99.5%), high PPV (99.0%) and high error (18.0%). False positive diagnoses were very minimal. False negative and inconclusive reports were seen from acellular aspirates from very hard lumps, haemorrhagic aspirates from highly vascular tumours and aspirates from cystic lumps. There was moderate agreement with histology (κ=0.64). Other studies showed similar findings.8,16-21,25, 26,22,23,24,25, On combination (The Triple Assessment) the methods concurred in 57% (114) of all patients. Concurrence was observed in similar proportions form other studies.10,16,21 When methods concurred there were no false positive and false negative findings. There was 100% sensitivity, specificity and accuracy 100%. Kappa statistic (κ) was 1.0 implying excellent agreement with histology. Similar observations of improved sensitivity, specificity and accuracy on the combined diagnostic methods were made in other studies. From the combination errors of individual methods get mutually cancelled and a definitive diagnosis was made with confidence, a view held by Kreuzer. The high errors of cytology and mammography limit their isolated10,16-20, 27, 28 29 Among the discordant results when two of the methods diagnosed malignancy, 93.5% were confirmed and when at least one method diagnosed malignancy 70% of them were confirmed. This suggested that if malignancy was one of the three diagnoses it could be upheld as further diagnostic evaluations are done. The concept of upholding the worst diagnosis is recommended by the breast cancer guidelines for Uganda.5 Conclusions and Recommendations Clinical diagnosis of breast cancer is of higher sensitivity than specificity and has high diagnostic error. Mammography and FNAC respectively have lower sensitivity than specificity but have high positive predictive values. When combined in the triple assessment, a definitive diagnosis can be made when the diagnoses concur, suggesting that the triple assessment has a high sensitivity, specificity, positive predictive value and negative predictive value with minimal error and excellent Kappa statistic. The output of the triple assessment in reproducible, making it a valid and reliable diagnostic approach to diagnosis of breast cancer. It is recommended that triple assessment should be practiced as the standard diagnostic method to diagnose of breast cancer. Definitive treatment can be started from diagnosis by the triple assessment before histology. The role of other radiological methods e.g. ultrasonography in the triple assessment should It is recommended that the triple assessment be evaluated to widen its scope and reduce its cost as a valid and reliable diagnostic method. References
© 2004 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js04052t2.jpg] [js04052t1.jpg] |
| |||||||||

{kind=link}
{kind=link}