 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 17-24 Improving Recruitment of surgical trainees and Training of Surgeons in Uganda M. Galukande1, S. Luboga2, S.C. Kijjambu1 1Department of Surgery, Faculty of Medicine, 2Dean’s Office, Faculty of Medicine, Makerere University Correspondence to: Dr. Moses Galukande, Email: mosesg@img.co.ug Code Number: js06005 Background: The surgical work output in Uganda is qualitatively and quantitatively inadequate. The number of surgeons is estimated at 100 for a population of over 26 million Ugandans. This paper reports on how to improve recruitment of surgical trainees and training of surgeons in Uganda, focusing on perceptions of potential trainees, trainers, and medical administrators.
Introduction
The Health workforce in Africa is grossly insufficient and poses a major workforce crisis1,2. The crisis includes lack of well-trained health professionals in the area of Surgery, under investment in the area of surgery does not help matters much because surgical conditions are unfortunately not seen as a public health threat and a general failure to recognize the importance of surgical care in the developing world3. The development of the health sector workforce in low-income countries has suffered from years of national and international neglect. This has become more apparent as new resources are being mobilized to fight HIV/AIDS, Tuberculosis (TB), Malaria and other diseases. Surgical conditions as a public health threat have been masked by HIV/AIDS, TB, Malaria, Acute Respiratory Infections (ARI), and diarrhoeal diseases among others. Lack of political commitment by governments and international agencies may be the single most important reason why surgical care has not progressed in developing countries. Surgery is considered to be too expensive as a treatment modality for the developing world4. Prompt and appropriate surgical care for many conditions such as trauma and hernia significantly reduces morbidity and mortality and can be a very powerful tool for poverty eradication. Surgical training is long and tedious. The workload is enormous and the pay is not so attractive in low resource settings. This could impact on the intake of surgical trainees. The surgical training for undergraduate medical students is not sufficient to enable the newly them once qualified to handle the challenges and workload that awaits them as general doctors. Over all, the surgical work out put is generally low in Uganda and East Africa. The personnel doing the work are not sufficiently equipped to do it, and what they do is qualitatively and quantitatively inadequate5, 6, 7. There is need for developing countries to revise general surgical training as a way of responding positively to the critical situation of low resources and low manpower8, 9. The aim of this study was to investigate factors affecting recruitment and training in surgery at Makerere University. Methods This study took place at the Faculty of Medicine, Makerere University, Uganda. It was a cross sectional descriptive study. Selfadministered questionnaires were used to gather information from intern doctors, Postgraduate surgical trainees, qualified surgeons and medical administrators. Focus group discussions were held for randomly selected members in each of the above categories save for the medical administrators after the questionnaires. The sample size was at least 50% for each category and included 25 of the 40 interns in Mulago national referral Hospital, rotating in the 4 major disciplines of Obstetrics and Gynaecology, Paediatrics, Medicine and Surgery, 9 out of 11 first year surgical trainees, 15 of the 17 second years and 6 out of 11 the 3rd year trainees. The issues addressed were the same in the questionnaires and focus group discussions. The data collected was analyzed manually. The study was approved by the Faculty Ethical and Research Committee (FERC). Results
Perceptions of potential trainees (Intern doctors) Twenty-one interns out of targeted twenty-five returned the self-administered questionnaires. For the second and third trainees, fifteen out of seventeen participated in the focus group discussion and filled in the self-administered questionnaires. Reasons for not choosing surgery as expressed by the potential surgical trainees included the high risk of acquiring HIV infection during clinical practice, the relatively heavy workload during training (academic workload and service workload) and the notion that surgery had limited career paths opportunities in the Makerere university and Mulago-Uganda setting when once one qualifies as a surgeon. Surgery was considered to be largely curative, does not lend itself to large scale preventive interventions, for that matter it does not attract large funding and attention (media, donors and governments); it is a poorly funded discipline relative to Paediatrics, Public Health, Medicine and Obstetrics and Gynaecology. Compared to other disciplines of medicine, in surgery there is less research activities which makes it less attractive for the research orientated or research aspiring individuals. The potential trainees suggested the following as means of improving recruitment:
Perceptions of current trainees (Post graduate students)
Ten out of fifteen first year trainees, the participants were engaged in a focus group discussion. The first year trainees gave the following as their reasons for having chosen surgery:
To improve on intake of students, they suggested that:
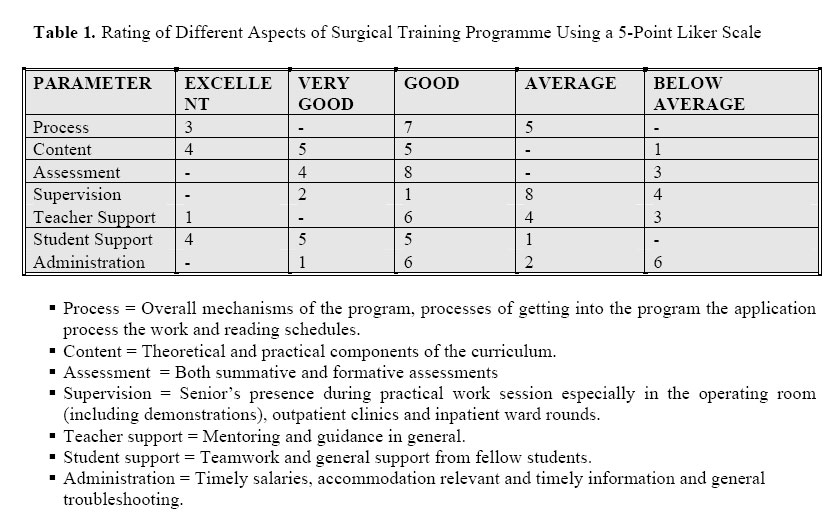
Table 1 gives a summary of the rating by trainees of the different aspects of the surgical training program. Weakness of current surgical training programme
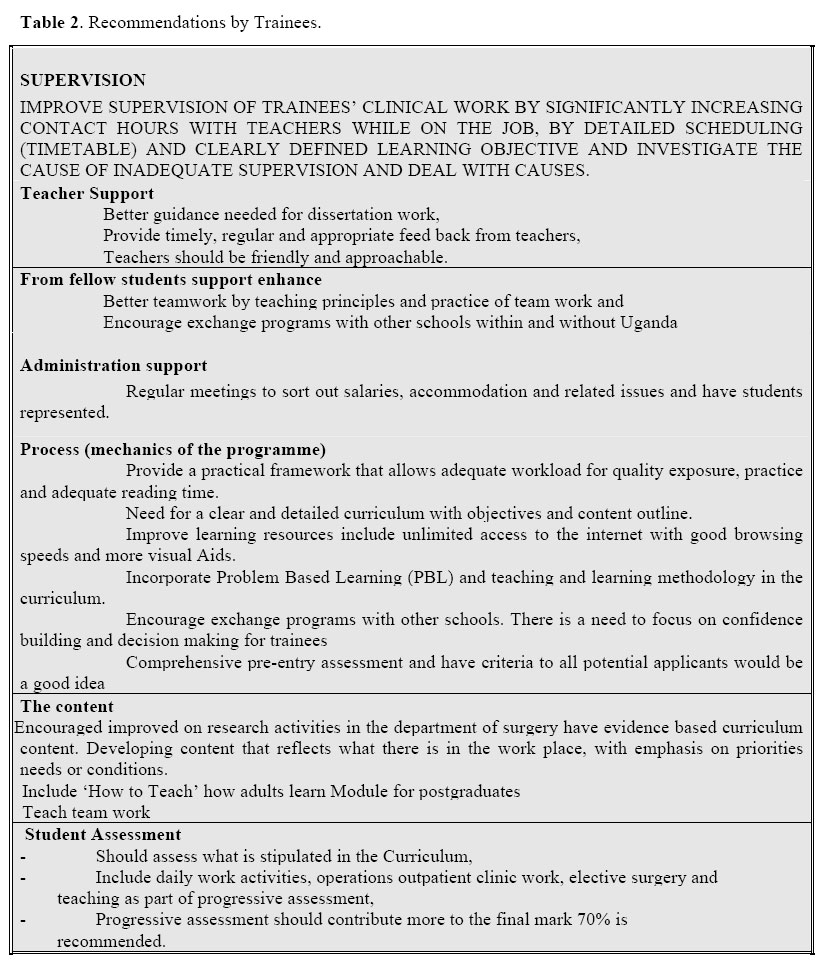
The recommendations by trainees on how to the Surgical Training Programme at Makerere University are improve summarized in Table 2. Perception of qualified surgeons Twenty randomly selected surgeons out of fortyfive in the Department, filled in a selfadministered questionnaire which was qualitatively analyzed, manually from a master sheet. Factors deterring recruitment of trainees for surgical training as perceived by the qualified surgeons were
Views on gaps in training The following views were seen as gaps by the surgeons.
Recommendations by surgeons to improve status quo
Key Informants (Teaching, Research, Fundraising and Medical administrators) Process
There are many unmet needs for the teachers in the faculty to make the process of learning for the students meaningful. These are leadership skills, managing staff, in-depth training in assessment methodologies and skills, curriculum development and evaluation and student counselling. Content
Need a curriculum review. At least after every five years to keep improving it as new evidence emerges from researches and informants (policy makers) as to what the priorities are. Assessment
Shift emphasis to progressive assessment, adopt new methods like OSCE (OSATS) (Objective Structured Clinical Examination) Teacher support and supervision
Most teachers are not trained to teach. They learn by apprenticeship and there is need to incorporate this in training and staff development. Staff Support
Redefine mentors’role and assign mentors earlier rather than later. Roles of mentor include helping out in dissertation writing. Administration A help desk for postgraduate students. Lobby government to pay more (high salaries) and levy fees from private students. Write proposals for Grants to support learning activities. Most of this money would be donor funds. There is under investment in education by government at the moment. Discussion
An international meeting on Human Resources for Health in Cape Town in September 2004 highlighted, the need for an urgent action to deal with the crisis of low numbers of trained personnel for health, requiring a concerted action of countries and all development partners. Surgical Training is severely constrained by under investment resulting in a shortage of almost all the facilities, infrastructure, beds and equipment. This situation is further compounded by extremely low numbers of trained personnel. Though this research focused on what could be done at a departmental level at the Faculty of Medicine, Makerere University to address Surgical Training Programs and the issue of shortages of trainee surgeons in Uganda, the solutions and efforts to effect, desirable change are also at two other levels; nationally at the Ministry of Health, Ministry of Education and globally with key players such as WHO, World Bank and IMF. Supervision
The critical areas highlighted are supervision and teacher support. Training in the tropics has enormous opportunities for hands on training and experience. There is a diversity of pathologies with opportunity to learn improvisation and adaptive skills. However, all this could be negated by inadequate supervision and demonstration of proper skills by the teacher to the student10. The trainers are few and overloaded with work. They are underpaid and poorly motivated and work in an environment that is inadequately equipped. The recommendations are possibly obvious to everyone:
To realize these recommendations a high level of commitment from the highest political authorities is essential4.
The teachers too should lobby the politicians more vigorously in order to realize a high level of political commitment and the funding that is likely to come with it. What would get teachers to find more time to supervise trainees? Teachers are generally paid inadequate salaries and they have to find other work (dual practice) to make ends meet reflecting the inability of Education and Health Ministries to ensure adequate salaries and favourable working conditions11. Does dual practice take away time and effort that should be spent supervising training activities?12 Competition for time is a nagging problem for many development agencies and Ministries of Health. There are simply too many meetings and workshops to attend13 in addition to private practice. Possibly trainees following teachers in their private practice for demonstration of patient handling skills and surgical skills could be a solution? Would formalizing dual practice generate a new commitment for teaching and supervision? Pretending that the problem does not exist or that it is a question merely of individual ethics or approaching it as a problem of corruption does not do justice to its complex nature and will not make it go away11. The earlier such an issue is comprehensively investigated and decisively dealt with the better. Preparation for teaching
The role of a Medical teacher is increasingly being recognized as a core professional activity for all doctors. Graduates must understand the principles of education as they are applied to Medicine. They must recognize the obligation to teach colleague. They must understand the importance of audit and appraisal in identifying learning needs for themselves and their colleagues.15,16,17 Medical schools should incorporate teaching and learning modules in both undergraduate and post graduate courses. Onsite training is also a good approach for those already in the business of teaching. Better pay
A widely advocated strategy for Human Resource for Health is to lobby government to appreciate the situational uniqueness of the workforce in Africa and remunerate it preferentially but this is faced with challenges. In the average low-income country, salaries would have to be multiplied by at least a factor of five to bring them to the level of the income from a small private practice 13,14. One of the ways worth exploring is the controversial question of introducing user fees, as a source of extra funding for health 18,19,20. Some of these funds would be paid to professionals who see patients and also teach. That user fees concept could be extended to increase the number of paying students (private students). Better facilities
It makes no sense to expect teachers to perform well in circumstances where the equipment and resources are patently deficient. Improving working conditions involves more than providing an adequate salary and right equipment; it also means developing career prospects, training and timely promotions. The Curriculum
The idea of having evidence based curriculum content entails findings out what conditions a health worker is likely to confront on a daily basis and train for that. The concept of defining core curriculum; must know, the nice to know and good to know follow. What is taught should be mostly a reflection of what is in the workplace. Conclusion
In order to accomplish the above there is need for better use of available resources. This however is not enough to achieve substantial improvement. More funding is required to recruit more trainees and therefore have more surgeons and surgeons that will stay. But as that happens we need more and better-equipped teachers. The realization of this requires strong commitment from all major players, preceded by strong advocacy and lobbying. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06005t1.jpg] [js06005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}