 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 25-27 VVF Treatment and Training through Outreach Services: AMREF Experience. Thomas Raassen, AMREF, Clinical Services P.O. Box 30125, 00100 Nairobi – Kenya. E-mail: raassen@wananchi.com Code Number: js06006 Background: In the rural areas, where the obstetric services are poor, where the woman has no say over her own body and pregnancy, where the husband and the family decide, what will happen with her? AMREF did a study and found that less than 15% of the referred patients in actual fact reach the referral hospital. For almost 50 years, (Flying Doctors Service) has been visiting remote government and mission hospitals all over Eastern Africa to bring specialist medical services to the sick. Introduction
Let me start by asking a simple question: “ Where do most of the women with Obstetric Fistula (OF) live?” The answer is obvious: “In the rural areas, where the obstetric services are poor, where the woman has no say over her own body and pregnancy, where the husband and the family decide, what will happen with her, when she goes into labour, where the 3 delays are prominent”. AMREF did a study and found that less than 15% of the referred patients in actual fact reach the referral hospital1. Is this strange? No of course; would you like to be treated in Moshi, when you live in Dar es Salaam? For almost 50 years, the Flying Doctors Service has been visiting remote government and mission hospitals all over Eastern Africa to bring specialist medical services to the sick. Over 100 hospitals are visited each once to six times a year. This service is done by plane: That might sound expensive, but it saves an enormous amount of time and is much safer than by road. If commercial airlines can be used, we do that. Since most hospitals are in the rural areas, the AMREF plane carries up to 6 or more specialists and drops them in different places. In 1992 after training in Addis Ababa, AMREF began to include VVF-repair in its specialist services. As it became known that something could be done about the obstetric fistulae (OF), hospitals were collecting more women for repair and new hospitals were asking for visits. During the visits the hospital staff developed interest and from that time onwards genuinely interested doctors got hands on training while the nurses received training in the pre-operative, perioperative and postoperative management of OF. A treatment protocol was developed as well as a simple questionnaire about the medical and social history of the woman. These visits have worked so well, that (after operation,) the women with repaired VVF are safely left in the capable hands of the local doctors and nurses. Once some doctors and nurses were trained in simple repairs, or were sent to Addis or Northern Nigeria for training, they continued doing the repairs in their own hospitals. In Tanzania for example there are now at least 12 hospitals, where repairs are being performed on a regular basis by specialists trained by and through AMREF. In Uganda 4 and in Kenya 2 hospitals are doing the same. Visits by the AMREF specialist to some of the hospitals in Tanzania continues for the more complicated cases, making teaching an on-going process. The same, but to a lesser extent is now going on in Kenya, Uganda and Somalia. A few of these hospitals could become training centres, as they have 2 or more specialists, doing repairs and because 150 – 250 repairs are being done per year, like BMC and CCBRT. In some of the larger hospitals VVF-workshops have been held. At the same time several specialists joined AMREF in visits to gain more experience (apprenticeship). The next step was to let trained specialists take part in the Specialists Outreach Program and operate and train on their own. Results In 2004 over 1300 VVF/RVF-repairs and related operations were performed in Eastern Africa by AMREF and AMREF trained specialists with 1 visiting English gynaecologist All the trained local specialists are performing VVF repairs. Many nurses have been trained in the management of OF Challenges
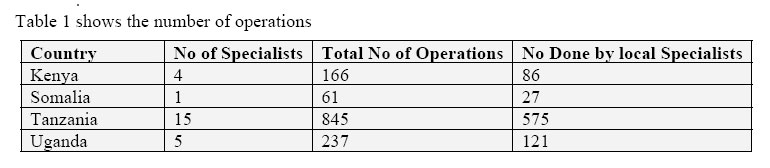
Over the last 25 years we have talked about prevention of maternal morbidity and mortality, under different jargon, like training TBA’s, Safe Motherhood, Reproductive and Child Health, and now Emergency Obstetric Care and it has cost enormous amounts of money. What are the results? Just look at these figures:
Many people in MOH’s, NGO’s, CBO’s, FBO’s and we do not know how many more O’s we will invent, have had a good salary and continue talking about and creating new ideas how to solve the problem. In October 2005, there was a meeting in South Africa, where UNFPA and other stakeholders were talking about the elimination of OF. At the start of the meeting a lady presented the Roadmap for Maternal and Newborn Health developed after the Millennium Development Goals for 2015 of the United Nations. After 25 minutes of talking with many slides, but none of the essential elements, like education, improving the infrastructure, building more health facilities, human resources development and paying the health workers a decent salary, somebody stood up and said: “My dear lady you talk about a Roadmap to fulfill these goals, but where are the roads to the non existent health facilities”? If we cannot solve the problem of prevention, let us then at least try to help the women with VVF/RVF and enable the doctors and nurses, dedicated to this work, to continue. Conclusions
The Way Forward
Reference
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06006t1.jpg] |
| |||||||||

{kind=link}