 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 28-31 Surgical Audit of Vesico-Vaginal Fistulae Repairs by on the Job Trained Medical Officers in a Rural Hospital, Kagando, Western Uganda.I.G. Munabi1 , T. Makumbi2, R. Sebwufu2, F. Mirembe3. 1 Department of Human Anatomy Makerere University Faculty of Medicine 2 Department of Surgery Makerere University Faculty of Medicine 3 Department of Obstetrics and Gynaecology Makerere University Faculty of Medicine, P.O.Box 7072, Kampala - Uganda Corresponding to: Munabi I.G, Email: imunabi@med.mak.ac.ug Code Number: js06007 Background: For each maternal death in Africa there are fifteen mothers who
suffer from some form of birth related injury, where the most devastating
form is the vesicovaginal fistulae (VVF). Teachings in most training centres
recommend that repair of these fistulae should be done by consultants. This
study aimed at evaluating the outcome of VVF repairs done by on the job trained
rural based medical officers in a rural setting. Introduction Annually 80% of the 50,000-100,000 women who develop an obstetric fistula during child birth are in Africai. The Vesico-vaginal fistulae (VVF) most commonly appear as a complication of delivery in 97% of the cases. It is expected that in East Africa, for each maternal death there are 15 mothers who suffer some form of obstetric morbidity the most common and most devastating being the VVF2. The VVF is a defect in the continuity of the epithelium creating a communication between the vagina and urinary bladder. This unnatural opening is the result of a series of events that lead to the death and sloughing off of the tissues between these two cavities. Among Africans VVF usually follows obstructed labour, which in itself is a result of a combination of factors which include poor childhood female nutrition, early marriage and pregnancy3, prolonged labour lasting several days sometimes, delayed or unavailable medical attention and extreme povertyii. The VVF has a very devastating impact on the life style of the afflicted mother. These women are frequently childless teenagers, divorced and considered as out casts in society due to their bed wetting and ever present smell of urine. As a result of this isolation these women at times never get to hear about the simple and effective operative repair procedure1 . The surgical repair of VVF involves the freshening of the defect edges followed by closure in layers. Successful repair are defined as a patient going home continent. There are many techniques that have been described else where with success rates ranging between 80%- 96% in some places4,5. The success rates are a measure of a unit’s surgical competence and to a smaller extent the quality of nursing care. The centres with the highest rates of success would ideally be the best for the repair this debilitating condition. The challenge is that for most of the affected women these centres are distant and expensive1-4. This paper explores the possibility of taking the service to these women within their communities through on the job training of communities through on the job training of community based medical professionals in Uganda. Methods This was a retrospective surgical audit for Vesico-Vaginal fistula repairs done at a rural 200 bed Kagando Hospital located 50 kilometres from Kasese town towards the Uganda -Democratic Republic of Congo border. The hospital is a non governmental, missionary hospital with a 30 year history of quality surgical care. It attracts patients from the whole of western Uganda, Eastern Democratic Republic of Congo and Rwanda. The hospital has a blood bank service, five wards and a two roomed fully equipped operating theatre. The hospital is run by a team of five medical officers two of whom perform an average two to three VVF repairs per week with or with out consultant supervision. The medical officers employed by the hospital are usually young university graduates with no more than one year of internship practice experience. The hospital has a strong culture of on the job mentoring/training of new medical officers by consultants and or more experienced colleagues. A manual search of the hospital’s archive yielded 112 patient records for a statistical 95% confidence interval, precision of 5 and power of 0.959. From the records an attempt was made to identify and record each patient’s demographic details, size and duration of the fistulae, pre, post and intra operative management and social issues related to the patient. During analysis defects of less than one inch in diameter were classified as small, and more than 1 inch in diameter as huge. The patient admission records patients for the third or more repair attempts were excluded from the study. Ethical clearance for the study was obtained from Makerere University faculty of medicine research and ethical committee. The research team also obtained permission from the hospital authorities before accessing patients’ records. None of the patient identifier numbers were used beyond data collection. Results
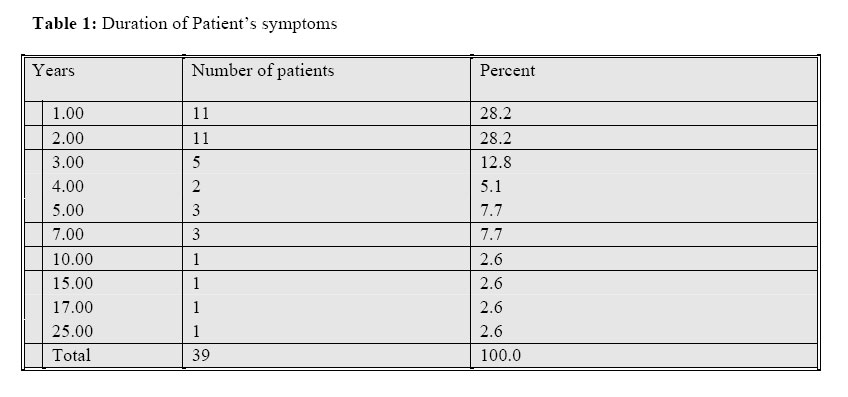
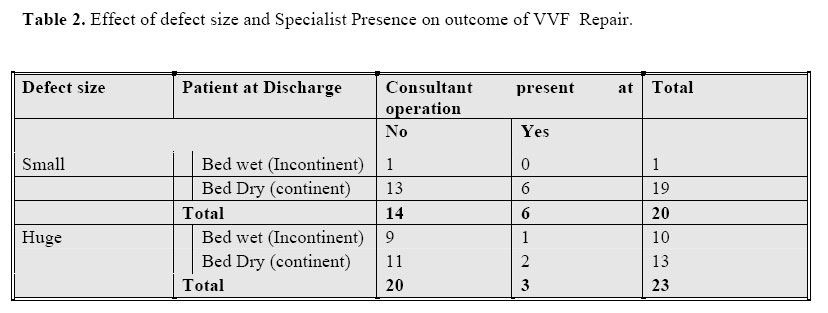
The ages of the patients treated for VVF ranged from 16 to 50 with an average of 25 years. The patients had an average of three pregnancies though sadly most of these patients did not have any children (15/32). Most of the patients had lived with the VVF for between 1 to 25 years with an average of four years (Table 1). At the time of coming to the unit most of the patients were still living with their spouses, (36/55, 65%). The most common presenting complaint was urinary incontinence reported in 88 (95%) out of 93 patients. Only 23% of these patients had received an attempt at defect repair (21/90). From the records, examination under anaesthesia revealed that, most of the patients had defects classified as huge (26/47). The majority of the repairs done by medical officers were successful (52/70, 74%). Medical officers had more success with the repair of small defects (Table 2), with no history of repair (small defects RR 1.69 CI 1.11-2.58). The repairs done by medical officers in the presence of consultants were more likely to succeed (RR 3.19 CI 1.90-5.53). There was no significant difference in the success of repairing huge defects by medical officers in the presence or absence of consultants (RR 1.21 CI 0.5-2.96). Only 19.4% (20/103) of the patients were able to pay the on average 200 US Dollar hospital bill. Discussion In Uganda and probably in most other developing countries, the teaching is that the repair of VVF should be left to consultants. These consultants are few and usually resident in busy national referral centres. In addition the VVF repair operation is very long as such these operations are avoided as they seem to take up valuable theatre space and nursing staff time1. The success recorded by the medical officers for these 70 cases shows that it is possible to repair VVF in these remote settings. There have been attempts to get around the challenges of time and nursing care. These include the development of dedicated repair centres as is seen in the case of the VVF centres in Ethiopia and India7. The problem with these centres is that in most cases they are beyond the reach of the dejected, isolated and impoverished VVF patients. In the case of Kagando a social worker used to collaborate and encourage the afflicted mothers to go for VVF repair. In spite of this there was a case of a woman who had a VVF for 25 years. Were this lady to fly to India she most probably would have opted to continue living with her condition. In Uganda the health system has been developed to a point where there is a fully fledged hospital with in the reach of most communities. The above results demonstrate that with some training and supervision medical officers can repair VVF’s. The success rate of 74% recorded for this health centre is certainly less than 80%96% seen at centres4,5. Probably with more training and supervisory visits this could have been better. In this audit only 19% of the patients were able to pay the hospital bills. Most were young with no children, and fortunately still married. With only 23% of the patients having had an attempt at repairing the defect, empowering the medical professionals close by with the necessary skills to repair VVF would help in two ways. It gives hope to the patient that the condition can be cured. Secondly it provides the community with an opportunity to learn about various safe motherhood practices thus reducing on stigma8. The strength of this retrospective study was affected by the challenges of accurate record making and keeping in a rural setting9. Despite these shortcomings, the successes of these on the job trained medical officers are worth noting. Giving hope, through education of resident doctors and the community, could reduce the stigma faced by these unfortunate mothers8. Conclusion and Recommendations In Uganda medical officers can successfully repair Vesico Vaginal Fistulae in rural settings with training/guidance. There is a need to equip community hospitals with the appropriate tools to repair this defect. The young Doctors should be encouraged and continuously supported to do the VVF repairs through regular supportive visits by VVF repair consultants. Acknowledgements Special thanks go to the staff of Kagando hospital, Dr. Bumbi Herbert the medical superintendent Kagando hospital, Mr J.B. Lwanga for the statistical help and Associate Professor Ely Katabira. This Audit was made possible thanks to a grant from Makerere Faculty of Medicine/SIDA-SAREC. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06007t2.jpg] [js06007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}