 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 32-40 Major Orthopaedic Procedures: 17 Year Trends.Biruk Lambisso Wamisho1, Woubalem Zewde2. 1Orthopedic Surgeon, 2Consultant in Orthopedic Surgery, Addis Ababa University - Ethiopia. Code Number: js06008 Objective: This study was aimed at determining the trends in the proportions of major orthopaedic procedures performed in the department of orthopaedics, Addis Ababa University in Ethiopia in the last two 'decades'. The factors contributing to the trends and their implications were also analysed.. Introduction
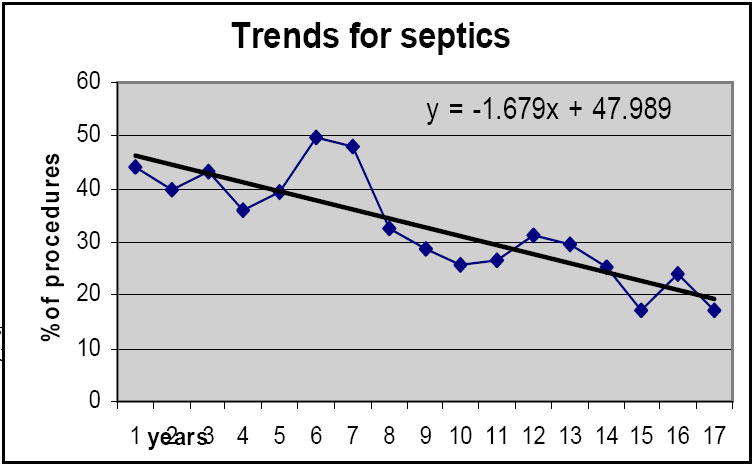
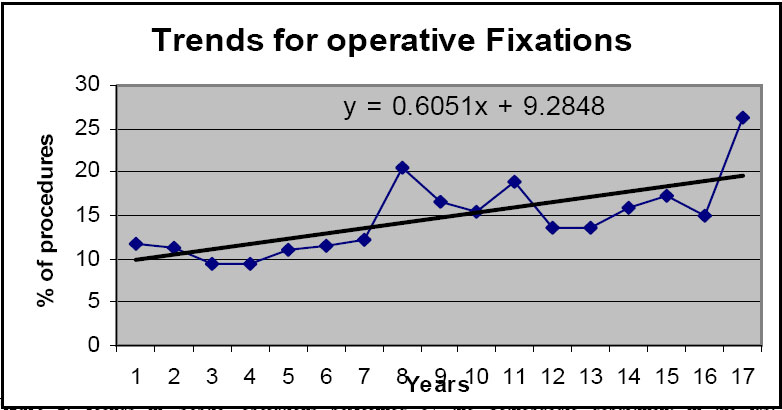
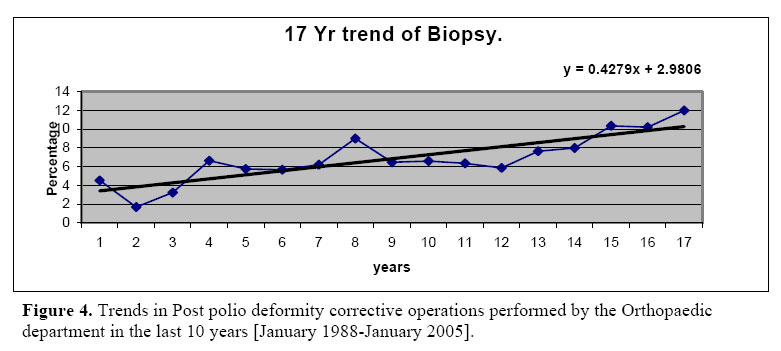
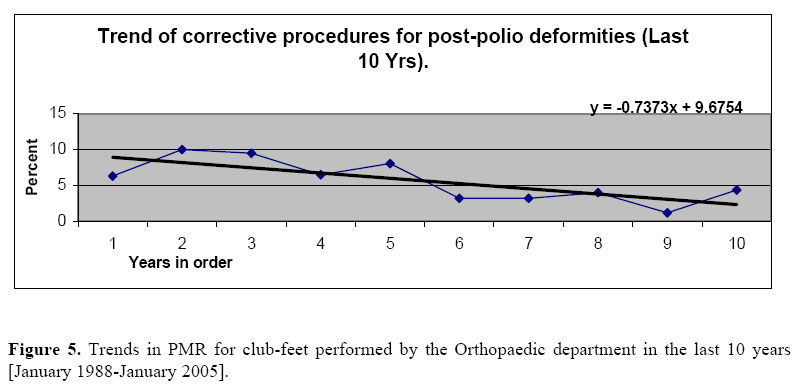
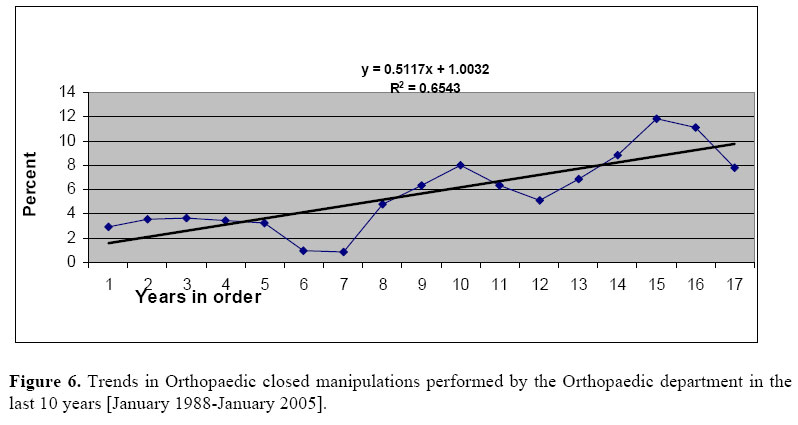
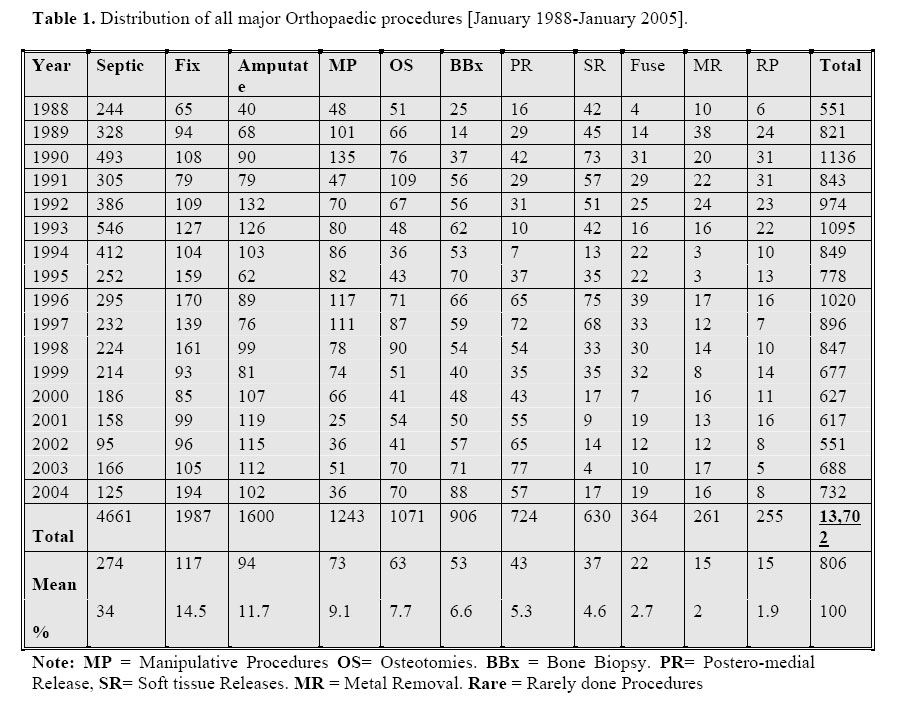
Clinical audit is perhaps the best-known example of the wider group of clinical effectiveness activities. It can be defined as the systematic and clinical analysis of the quality of clinical care including the procedures used for diagnosis and treatment, the associated use of resources and effect of care on the outcome and quality of life for the patient1. The primary function of clinical audit is to improve patient care by informing healthcare professionals’ understanding of their practice. This is usually achieved by setting standards, measuring current performances, observing trends, identifying pitfalls and putting in place any necessary actions1. In essence, clinical audit aims at establishing the extent to which the actual practice compares to the standard established by clinical research. As standards change often, re-audit may be necessary. Audit is a continuous process by which practice and care are improved. Many developed nations have well-structured and budgeted audit systems, such as the Clinical Resource and Audit Group (CRAG) of Scotland2. This however may be impossible in very poor countries like Ethiopia. There are financial and logistic constraints with poor compliance of patients for follow-ups. Consequently, retrospective observations of trends remain an important tool and feasible pointer of future directions in the developing countries where more than 80% of the population of the world and a vast reservoir of orthopaedic pathology are located. More than 80% of deaths in road traffic accidents and 90% of those involving children occur in developing nations3. This results in large number of patients demanding some form of orthopaedic operation. Added to this are industrial and fall injuries. Many developed nations have well-structured and budgeted audit systems, such as the Clinical Resource and Audit Group (CRAG) of Scotland2. This however may be impossible in very poor countries like Ethiopia. There are financial and logistic constraints with poor compliance of patients for follow-ups. Consequently, retrospective observations of trends remain an important tool and feasible pointer of future directions in the developing countries where more than 80% of the population of the world and a vast reservoir of orthopaedic pathology are located. More than 80% of deaths in road traffic accidents and 90% of those involving children occur in developing nations3. This results in large number of patients demanding some form of orthopaedic operation. Added to this are industrial and fall injuries. Trained orthopaedic surgeons are desperately needed in developing countries but their provision in a poor country raises another issue, the cost. Modern orthopaedic surgery is very expensive. A highly trained and active surgeon will get frustrated working in a country where a simple plate with six screws costs more than the annual health budget for ten people. This encourages the use of less costly conservative methods of treatment. Often these are appropriate, but sometimes they are second best, and it is a struggle not to compromise the quality of care. Salaries paid by governments to specialists in developing countries are often insufficient to keep family fed, let alone cover school fees and buy cars4. Even though orthopaedic surgeons have the greatest caseload and time load, most orthopaedic surgeons have to undertake private practice just to survive5,6. Thanks to the material support in the form of donated orthopaedic equipment, the training environment of residents in developing world is going a long way. Of course, as this is not sustainable we are sometimes forced to re-use implants. Sometimes certain operations are not done due to constraint in implants and the trainees may never be exposed to such procedures as they are assigned to less equipped district Hospitals. Orthopaedics in developing countries like Ethiopia is in a struggle between the demanding patients on one side and the equipment constraints on the other side. This study was aimed at observing the pattern and trends in orthopaedic procedures performed in the past two decades at Addis Ababa University, Medical Faculty, Department of Orthopaedic Surgery, 'Tikur Anbessa' Hospital (Black lion Hospital), the only orthopaedic speciality training department in Ethiopia, enormously supported by the U.K. and U.S. Possible solutions to the problems of orthopaedics in developing countries are presented. Patients and Methods Records of all major orthopaedic procedures performed in the Department of Orthopaedics Addis Ababa University, Tikur Anbessa (Black lion) in the last 17 years from January 1988 to January 2005 were reviewed. The hospital is a tertiary level teaching hospital of the University’s Medical faculty. The orthopaedic department is the only orthopaedic specialitytraining department in the country. After getting approval of the study from relevant authorities, all the records in the operation room registry (logbook) were checked by the investigators. All military patients and minor operations were excluded from the study. Operationally, major Orthopaedic procedure was defined as an Orthopaedic procedure performed on admitted patient on a major bone, major joint or lasting more than an hour. There were over 40 different types of procedures, which were regrouped into 10 similar categories for easy handling of the data. All the variables on the register were analyzed. Forty-six wrong registrations were excluded. Data analysis was done by Excel- 2003, Microsoft office software. Significance tests and trend equations were calculated by EpiInfo-2002 Version 6 software. Results A total of 13,702 (806/Year) different major orthopaedic procedures were performed by the department in the last 17 years. The distribution of the forty different types of procedures is shown on Table 1 after they were regrouped into ten major categories. The mean age of adult patients was 34 years. Males accounted for 10,140 (74%) making the male to female sex ratio 1 to 3. Children (age <14) were 3,974 (29%). Trauma was the cause in 65% of the procedures and over 80% of the procedures were done on elective basis. Emergency surgery was done on 2,603 (19%) of the patients. On the average two emergency patients that must have been operated were referred to other Hospitals due to lack of bed, and about 700 emergency patients were missed every year. On average patients waited for five weeks before getting beds, for ten days before getting operated and for three weeks before discharge from the wards. The commonest operations were septic procedures, 4661 (34 %). A little over half of this was debridement; about a quarter were varieties of secondary wound closure; incision and drainage of abscesses accounted for 10%, and 5% of the septic procedures were on acute joint infections. There were 1,987 (14.5 %) fixation of fractures (Table 2). External fixation accounted for 109 (10%) of the fixations and the rest (90%) were internal fixations. Slightly over half of the internal fixations were open reductions of fractures and internal fixations using different plates, screws, pins and wires. Intra-medullary nailing (IMN) accounted for 172 (8.6%), tension band wiring (TBW) for 302 (15.2), and hip fixations for 254 (12.8%) of fixations. Of the procedures on hip, hemiarthroplasty was performed on 48 (18.8%) of the 254 the patients. Total hip replacement was just started in year 2005. There were no knee replacements. There were 1,600 (11.7%) amputations, the most common amputation being below knee amputation (30 %). This however changed to above knee amputation (AKA) in the last few years (Fig 7), usually due to diabetic complications. The main indications for amputation were trauma (55%), complicated diabetes (17%), tumours (12%) and traditional healers (4.2%). Bone biopsy was done in 906 (6.6 %) of the patients. Procedures to correct post polio deformities included triple fusion (2.2 %), osteotomies (3.9 %) and simple soft tissue releases (3.8 %). Postero-medial release for clubfeet correction was done in 724 (5.3 %). Closed manipulations were done for 1,243 (9.1 %) of patients. ‘Major’ (big) implants were removed from 261 (2%) of the patients. Most of the removed implants were reused. Despite the availability of good number of patients, operations for correction of congenital hip dysplasia (CHD), on the spine and on the shoulder were done very rarely. Trends observed Over the years under review, number of major procedures on admitted patient steadily decreased. An increasing trend in numbers of operative fixations, amputations (except BKA), PMR and bone biopsy was observed. A decreasing trend was seen in septic procedures, closed manipulations and procedures for post polio deformity correction. Chi-square for trend of Operative fixations is 105.54 (p<0.001) and the increasing trend is statistically significant, for bone biopsy it is 93.9 (p<0.001), statistically significant increasing trend, and for PMR also the increasing trend is statistically significant (chi-square 153.81). Statistically significant decreasing trend was seen for septic procedures (chi-square 395.44), post polio procedures (chisquare 64.25). All the conditions remaining the same; the proportion of operative fixations by the year 2015 is predicted to be 26.1 % and after fifty years half of the procedures will be fixations. This was calculated from the linear equation of the straight trend line on Fig-I (y= 0.6x + 9.3). Where, ‘y’ is the percent and ‘x’ is the year order. Similar useful equations and predictions can be derived from the remaining trend lines (Figure 2, 3, 4, 5, and 6). Discussion Findings from this audit present an insight to the operative trends in our set up & similar institutions in developing countries. The following findings are similar to comparable population in other developing country cities: relatively young (mean age 34 Years), predominantly male (Three fold) sex and commonest causes of operation trauma. (6, 7) It had been our impression that most of the documentations could be lost, but all were available despite the poor recording systems we have. This may be due to the fact that extra care is given to operation room documents as they may have legal implications. The theatre registry lacks variables that provide information to assess the training, caseload, time load and workload. This is also a problem even in highly developed countries. (8-11) The number of emergency patients referred-back due to lack of bed (700/ year), the duration on admission waiting list (5 weeks), the length of hospital stay (three weeks) and the ten days stay (after admission) waiting for theatre schedule are rather depressing figures as compared to developed country standards of few days12,13. Besides lack of bed, patients are referred to any hospital or abroad, due to lack of equipment and senior staff. Septic/ unclean procedures like debridement and abscess drainage are the most frequent operations done (34%) but they have shown a steadily decreasing trend with a negative slope (Figure 2). This is ‘good news’ and the reasons may be the cessation of the protracted civil war the country was undergoing, improvement in primary health care and early referral systems. On the contrary, it can be due to failure to admit emergency trauma patients during the golden hours. Operative fracture fixations of different types have shown a sharp increase (Figure 1). This is for internal fixations and external fixations, which account only for 10% are decreasing (Table 2). Hip surgery is currently practiced frequently, with the aid of C-arm and donated endoprosteses. This needs particular attention, as the current tendency towards operative fixations will face a problem for the equipment is unaffordable to our patients. We are sometimes forced to reuse donated metals from the developed world. Without donations of highly demanding and expensive orthopaedic equipment by developed nations, modern orthopaedics and training in developing countries will be unthinkable. (4) Arthroscopic surgery is in its infancy. Hand & spine major operations are operated by separate specialities and are not included. Amputations are the other commonly & increasingly done operations. This could be due to increase in the causes. For example, an obvious increase in bone biopsy for tumours is observed (Figure 3). In the last few years, AKA has became the most frequent amputation in diabetics, this is due to the use of Doppler ultrasound to localise the level of vascular obstruction, in our case, which is usually in a proximal big vessel. Disappointingly most of our amputations were preventable. (14,15) Operations to correct residual deformities from polio infection, for example triple fusions, osteotomies and soft tissue releases have shown decreasing trends, especially in the last ten years (Figure 4). This can be explained by the fact that extensive national polio eradication campaigns were taken in the country. There is also an increase in the vaccination coverage. The commonest paediatric operation is PMR for clubfeet and it was increasingly done (Figure 5). This is contradiction to international standards, which declare that surgery is a wrong approach to clubfoot18. Dr. Ignatio Ponseti’s conservative clubfoot treatment method that we are using now, together with a falling trend in closed manipulations (Figure 6) will avoid unnecessary admissions on already scarce number of beds. The manipulations can be done as day –case or short-stay procedures. (16,17) This makes more beds available for waiting patients. Some operations are rarely done and are usually done by visiting consultants from developed countries. This may bring improper case-mix to the trainees, as some may even never attend the operation in the whole residency period19. Orthopaedic practice is dynamic20. Over the seventeen-year period, a decreasing trend in the total number of operations is seen (Table 1), this could be explained by the fact that relatively sophisticated (Internal fixations) and time consuming operations are increasingly done. This results in fewer numbers of operations to be performed each day and variation in casemix18,19. The limitation of this study could be the fact that it was retrospective, but it has also a strong point –it observes a trend over two decades. To the best of our knowledge, there is no similar study has been done in Africa. Therefore facts drawn from this study will be very important informative of what is going on in the developing world general orthopaedics. Conclusion There were significant shifts in Orthopaedic operative trends over years. This shift was mainly towards operative treatment of fractures which demands a lot of imported expensive implants. Developing countries like ours should look for a means to satisfy these demands. Acknowledgment We are indebted to the Dr. Stephen K. Wood, Dr. Tezera Chaka and Prof. Geoffrey Walker for their marvellous assistance. We thank Dr. Tesema Ersumo, president of SSE and Prof. D.B. Jones for their assistance in editing our presentation & manuscript. We appreciate the assistance we got from our medical director, Dr. Zereu G. and our OR head nurse, Sr. Tewabetch for letting us use the all the documents they safely kept for two decades. Finally we acknowledge the constant encouragement and support we received from our families. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06008f2.jpg] [js06008f6.jpg] [js06008f1.jpg] [js06008t2.jpg] [js06008f8.jpg] [js06008f5.jpg] [js06008f4.jpg] [js06008f7.jpg] [js06008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}