 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 41-48 Permanent Civilian Musculoskeletal disability following injury-17 Year trends. Lambisso W. Biruk1, M.D, 1Orthopaedic Surgeon, Addis Ababa University, Medical Faculty,
Orthopaedic department, Ethiopia. Code Number: js06009 Background: This study was aimed at determining the magnitude of civilian permanent
musculoskeletal disability from injuries and identifies trends observed in
the proportions of major causes of the disability in the last two 'decades'.
Introduction World health organization (WHO) defines disability shortly as any restriction of ability to perform an activity in the manner or within the range considered normal for a human being. It is a gap between what a person can do and he needs to do. American Medical Association (AMA) defines it, as a condition that interferes with individual's activities of daily living. Disability percentages are used to estimate the degree to which an individual's capacity to carry out daily activities are diminished (1). Changes in lifestyle, urbanization and socio-economic developments in recent decades have caused changes in disease and disability patterns due to rise in incidence of non-communicable disease and injury among the youth in developing countries (2,3). Globally, injury has become a recognized health problem with a steadily increasing trend. According to WHO and World Bank projections, injury is likely to account for 20% of the disease burden on the world population by 2020, with road traffic accidents (RTA) alone being the third leading cause (4-8). It ranks third behind diarrhea and malaria in Africa (9). In the economically active age group, RTA is the leading cause of death only next to HIV/AIDS but has got less attention (10). This is specially the case in country (like ours) where there is a recent increase in Industrialization and motorization (11-15). The burden will be equal to that of communicable diseases, and greater in some developing countries. Every day about 16,000 people die from injury and obviously, for every death from injury, there are thousands of permanent disabilities. Musculo-skeletal problems are extremely common and have a substantial influence on health, quality of life and resource allocation. This is a Bone and Joint Decade with a noble global goal to improve the health related quality of life of people with musculo-skeletal conditions by raising awareness of the suffering and cost to the society resulting from the problems. Of course, this needs empowering patients to participate in their care, implementing cost-effective preventive measures and promoting research to improve prevention and treatment (16-18). Pattern of muskulo-skeletal disability differs from place to place. In Ethiopia, injury is a major health problem accounting for more than a quarter of all surgical admissions, deaths or disabilities (1922). In the past decade, Sub Saharan Africa reported to have 42% increases in the road fatalities and road traffic accidents are the commonest causes of trauma in urban Ethiopia with 199 fatalities per 10,000 registered vehicles per year (23-25). Disability evaluations need careful assessment and long-term follow-ups to reasonably estimate the percentage of permanent impairment. Added to this, issues of employability, claims and litigation demanded more from the health system. Indirectly, magnitude and pattern of disability data can be used to evaluate the efficiency of a health system. Identification of important causes of permanent disability can help policy makers and stakeholders to address the problem systematically. Hospital data can be a useful tool for assessing disease Epidemiology in a population. Even though the data is of a small scale, substantial insight can be made into the major causes of permanent musculo-skeletal disability and the trends in proportions over several years. Almost all studies in Ethiopia combine orthopedic (muskulo-skeletal) conditions with general surgical conditions, and this has lead to underestimating of the burden of muskuloskeletal problems on our society. Added to this, the rampant visits to traditional healers and limited access to modern health facilities and insurance companies will make the condition worse. Our audit was approved ethically and there are no conflicts of interest. It aims at determining the pattern magnitude and trends of major musculo-skeletal disability causes with relevance to future preventive interventions. Methods Patients: The documents of all injury patients assessed by orthopedic medical board at TAUH in the study period [1988 - 2005] were audited. Disabilities not from musculo-skeletal injury and patients assessed by other medical boards were excluded. All of the patients were civilian and military patients were excluded. All the relevant authorities were informed and gave permission. Setting: TAUH is a tertiary level teaching Hospital located in the capital and serves the whole country of over 70 million inhabitants. It is the only hospital in the country with a teaching orthopedic department. On average 806 major operations are done per year and over 60% of this patients are admitted due to trauma. The department receives every year, on average 15,621 follow-up visits and 3,200 emergency patients. About 13% (560/71) of its beds are allocated for orthopedic patients. The orthopedic medical board is composed of three senior orthopedic consultants and the Hospital's medical director. One of its activities is to assess applications of disability and award percentages, using different available schemes including the American Medical Association’s disability evaluation Guide and 4-5 applications every week are evaluated. The applicants have to pay 35 USD for each evaluation. The applicants are provided with copies of the board’s decision so that they can take it to insurance companies, to the court or to other compensation institutions including the government. Design: The investigator reviewed all the documents. Parameters like cause of the injury, site of injury, percentage disability awarded, duration of the injury and the final recommendation of the board were tallied. Repeat applications were identified and audited in detail. 'Permanent' musculo-skeletal disability from injury was defined as a stable (non progressing) impairment resulting from an injury on the one of the musculo-skeletal structures. Statistical Analysis: The data were entered; cleaned and analyzed using Epi Info-2002 version 6 and MS-Excel 2003.Appropriate significance tests and trend equations were also done. Results
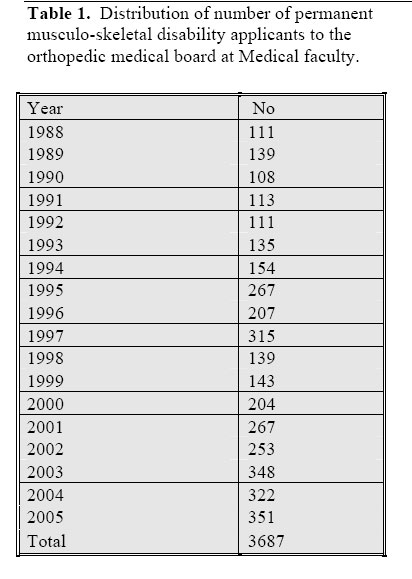
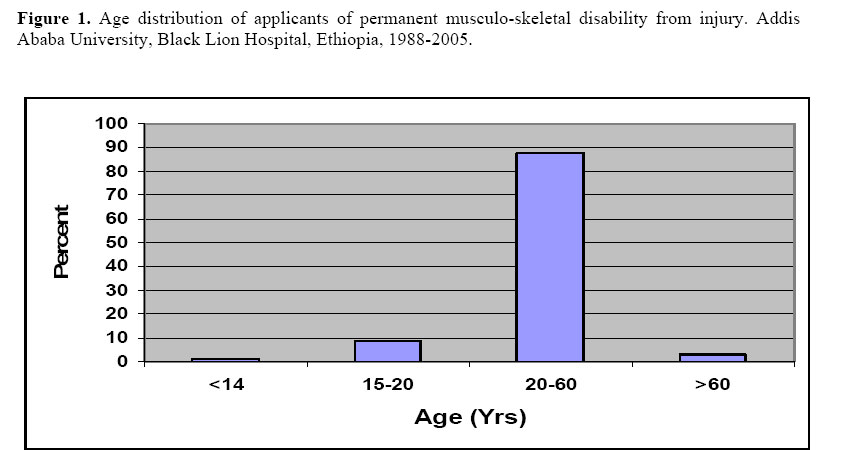
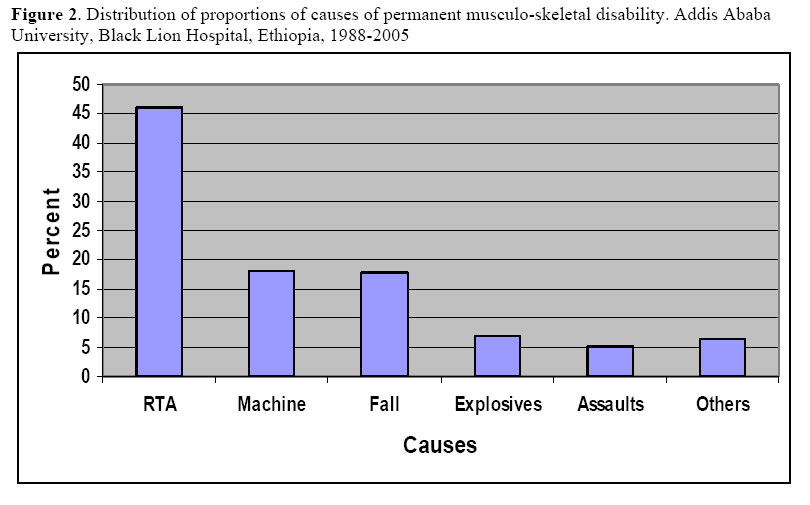
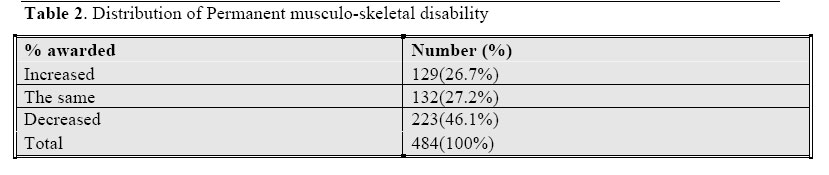
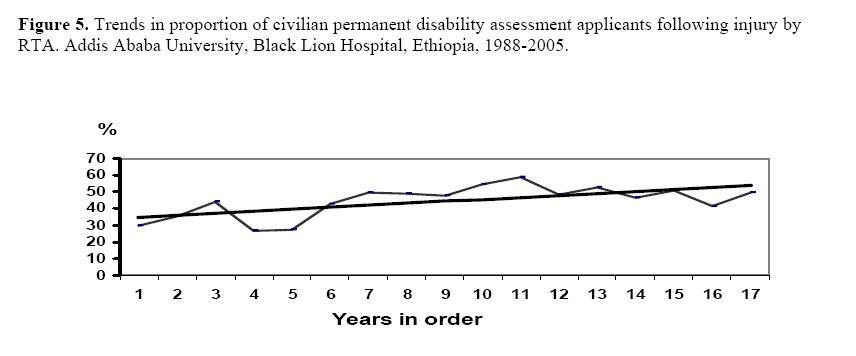
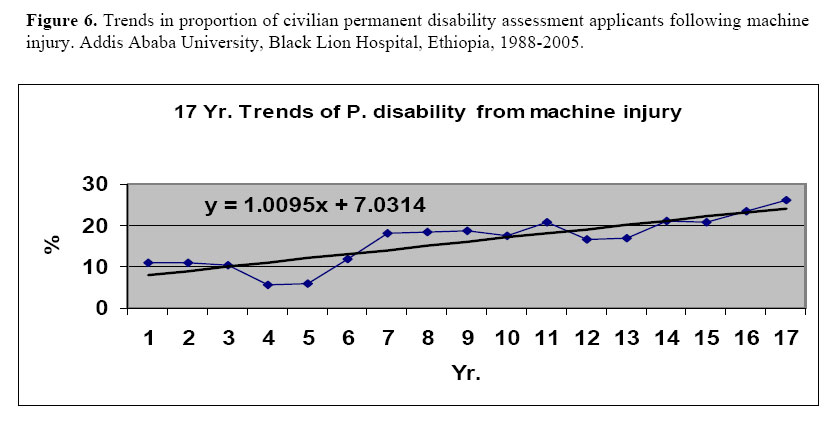
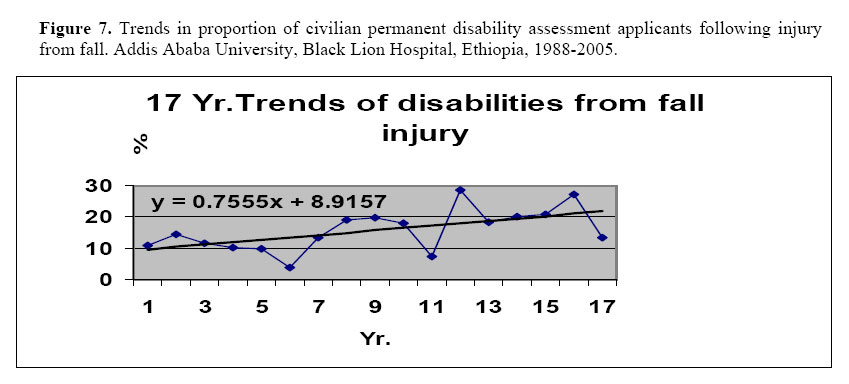
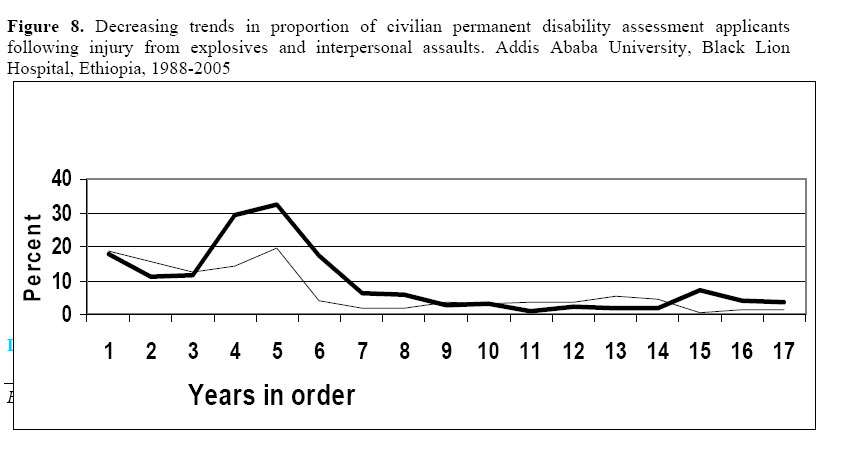
Sociodemograpy: A total of 3,971 (221/Year) civilian musculo-skeletal ‘permanent’ disability applications from injury were reviewed by the orthopedic medical board of the Hospital in the last eighteen years (Table I). Two hundred eighty four (7.1%) had to be excluded from this audit, as there records were either incomplete or the documents are unreadable. The patients came from all over the country but most, (3,245 (88%)) were from Addis Ababa. All but 708 (19.2%) of the patients were treated in our Hospital. The majority (87.4%) of the applicants were from the working age group of 20-60 years. (Fig 1). The mean age of the applicants was 28 years (Ranges from 8-77 years) and the frequently affected age was 25 year. Three thousand two hundred sixteen (81%) applicants were males making the male to female sex ratio 4:1. Road traffic accident (RTA) was the cause of disability in about half of the applicants (1827/3971, 47%) and over 80% of these are ‘hits by cars’ (Pedestrian injuries). Machine injuries and falls from height, each accounted for 18% of the proportion. The remainder proportion was shared by interpersonal assaults, explosive injuries and others (Fig 2). The commonest sites injured were the hand (26%) and the leg (12%). Dominant hand was injured in 60% of the hand injuries. Injuries on the upper limb accounted for 1880 (51%) and lower extremity injuries accounted for 1401 (38%). The rest were poly-trauma (8%) and spinal injuries (3%), Sixty percent of the applicants presented with in less than six months of the injury and only 553 (15%) applied after a year. Reapplications and reassessments were made by 484 (14.9%) and 93% (450/484) of these have made their first applications in less than four months of the injury. Only sixteen patients applied for a third time. The outcomes and reasons for these applications were shown in (Table II). A little over half of the applicants were awarded a percentage whole person disability of less than 10%. The board awarded >75% for eighty eight applicants. Trends observed: In the decades, number of applications for assessment of disability is steadily increasing. An increasing trend in proportion of permanent musculo-skeletal disability applicants from RTA, machine injury and fall was observed. Chi-square for trend of RTA was 11.8 (p<0.001), for machine injury it was 24.1 (p<0.001) and for fall also the increasing trend was statistically significant. All the conditions remained the same; the proportion of the applicants from RTA by the year 2015 is predicted to be 67.3% (Two third of all applications). This is calculated from the linear equation of the straight trend line on Fig V (y= 1.2x + 33.7). Where, ‘y’ is the percent and ‘x’ is the year order. Similar useful equations can be derived from the remaining trend lines. On the contrary, proportion of civilian disability applicants due to injuries from explosives and assaults has shown statistically significant decreasing trends. (Figs 5, 6, 7 and 8). Discussion
Findings from this audit present an insight to the consequences of musculo-skeletal injury in our set up. The following findings are similar to comparable population in other developing country cities: relatively young (mean age 28 Years), predominantly male (Four fold) and commonest causes RTA and fall19,26. It had been our impression that most of the documentations could be lost, but all were available despite the poor recording systems we have. This may be due to the fact that extra care is given to medical board documents as they have legal implications. The majority (87.4%) of the applicants were in the working age group (20-60 years), this is in consistence with other reports and augments the burden of HIV/AIDS2,3,10,19 set up. The following findings are similar to comparable population in other developing country cities: relatively young (mean age 28 Years), predominantly male (Four fold) and commonest causes RTA and fall19,26. It had been our impression that most of the documentations could be lost, but all were available despite the poor recording systems we have. This may be due to the fact that extra care is given to medical board documents as they have legal implications. The majority (87.4%) of the applicants were in the working age group (20-60 years), this is in consistence with other reports and augments the burden of HIV/AIDS2,3,10,19. Road traffic injuries are the commonest cause of permanent musculo-skeletal disability applications (47%). This is not surprising as road traffic accidents are the commonest causes of injury in Addis Ababa roads with 199 fatalities per 10,000 licensed vehicles per year (highest in the world)27. In the past decade, the case fatalities increased by 42% and some recommended even not to derive in Ethiopia24. Most of the RTAs are pedestrian injuries and were caused by commercial vehicles and are possibly preventable. This is in agreement with other studies in Ethiopia6,28. The same study has shown that in semi-urban and rural Ethiopia the commonest cause of injury is interpersonal assault and RTA ranks third. Machine injury and fall from height at constructions, in increasing proportions are ‘newly emerging’ causes of disability in our country. This may be related to the current increase in the construction work and the industry-centered policy the country is following. Luckily, applicants due to injuries from electric accidents were very low (<1%) and burn injuries were not seen because there is a separate burn center in the city to deal with all sorts of burn. This may be due to the limited access to and utilization of electric power. Injuries from assaults and explosives have shown a decreasing trend in the decades and we are ‘sleeping well’, this could be due to the cessation of the protracted civilian war the country was facing, a result of tighter firearm control systems and improved law enforcement. Exceptions to this are years 1990 and 1991(see all the downward indentations in all the trend graphs), where there was an exchange of governments in the country with all the aftermaths. Overall, an increasing trend in the number of applicants for disability assessment was observed and this could partly be due to an increase in the major causes of musculo-skeletal disability, an increase in number of insurance/work related compensation companies (from 1 to 8, which is still very low as compared to developed nations29,30 in the country or due to an increase in awareness among the population. Nearly all the applicants came due to traffic accidents, machine injuries or falls. The trends have kept steadily increasing, and predictive equations derived from the decade’s observation should alert policy makers. It is known that as this is a hospital based study, the magnitude of injury could be underestimated since all individuals with injury might not present to a health institutions due to low health service coverage, poor income and preference to local healers However, the study provides some valuable information and the fact that permanent disability is one of the final consequences of injury, conclusions drawn from this will be very important indicators. Based on the study the following series of recommendations are forwarded:
Acknowledgments
The author is indebted to Dr. Stephen K. Wood, Dr. Tezera Chaka, Dr. Paul Baxt from Orthopaedic Overseas-U.S, Mr. K. Tuson from WOC-UK and Prof. Geoffrey Walker for their support, to Dr. Tesema Ersumo, President of SSE for his help in editing our presentation & manuscript. We acknowledge the assistance we received from our medical director, Dr. Zereu G. and our Departmental Secretary for safely keeping the records for two decades. Finally to my wife, Sr. Lili and our families for their persistent encouragement and prayers. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06009t2.jpg] [js06009f5.jpg] [js06009f8.jpg] [js06009f1.jpg] [js06009f2.jpg] [js06009f6.jpg] [js06009f7.jpg] [js06009f3.jpg] [js06009t1.jpg] [js06009f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}