 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 57-61 Giant Ulcerative Lactating Nodule of Ectopic Breast Mimicking Malignancy.I. Roy1 FRCS(C), E Othieno2 MMed (Path), R Ssentongo3 FCS (ECSA) 1Department of Pathology, St. Raphael of St. Francis Hospital, Nsambya, Kampala, Uganda and. Department of Pathology, St. Mary’s Hospital, McGill University, Montreal, Canada, 2Department of Pathology, Mulago Hospital, Kampala, Uganda, 3Plastic and Burns Unit, Mulago Hospital, Kampala, Uganda- RS). Correspondence to: Dr. Indrojit Roy. E-Mail: indrojit_roy@yahoo.ca Code Number: js06012 Objective: Lactating nodules occur in the pregnant and post partum patient and require investigation to rule out the possibility of a malignancy The aim of this paper is to document occurrence of a rare case of ectopic breast mass in a post-partum woman that mimicked malignancy and proved to be a diagnostic challenge both clinically and cytologically, in order to sensitize physicians to such cases. Introduction
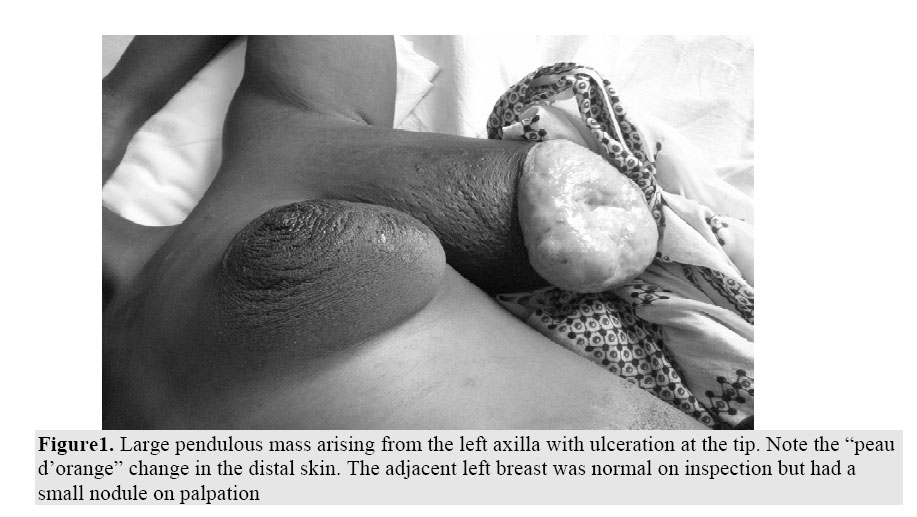
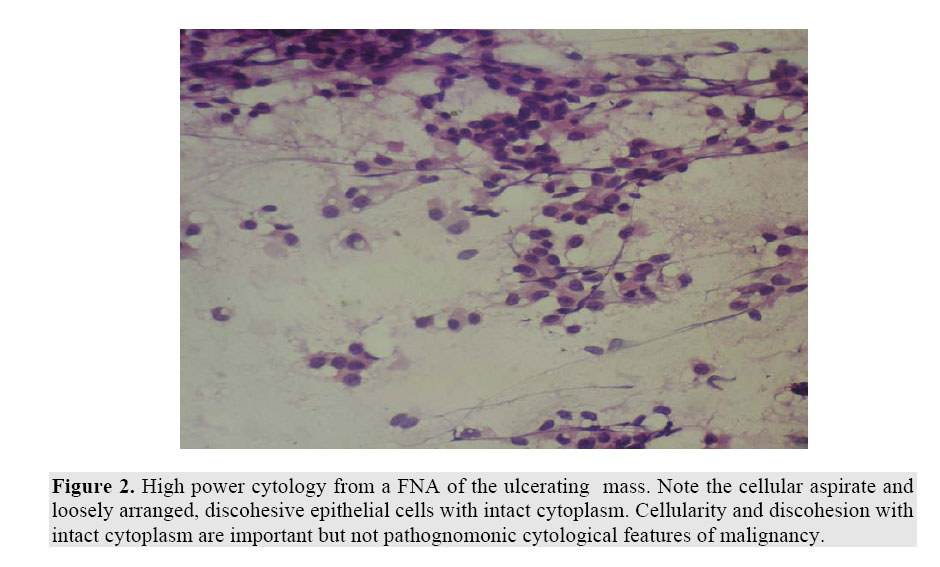
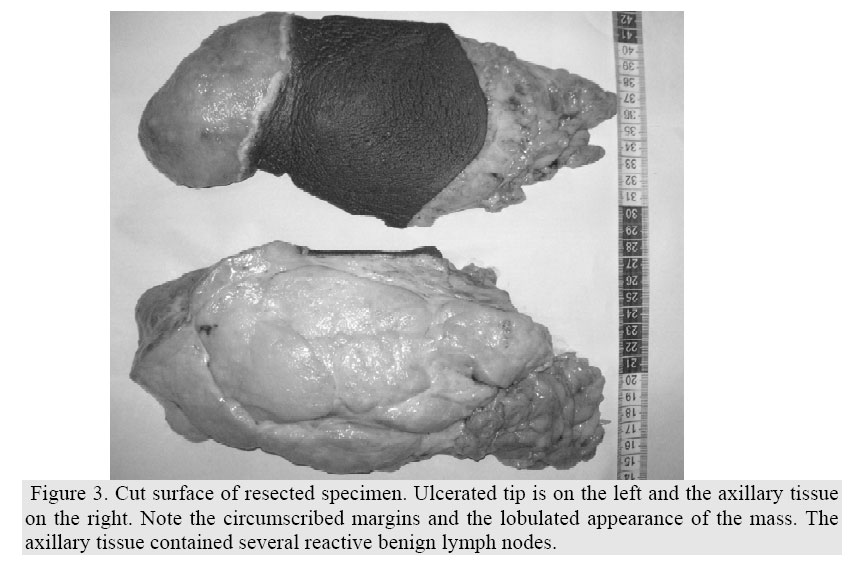
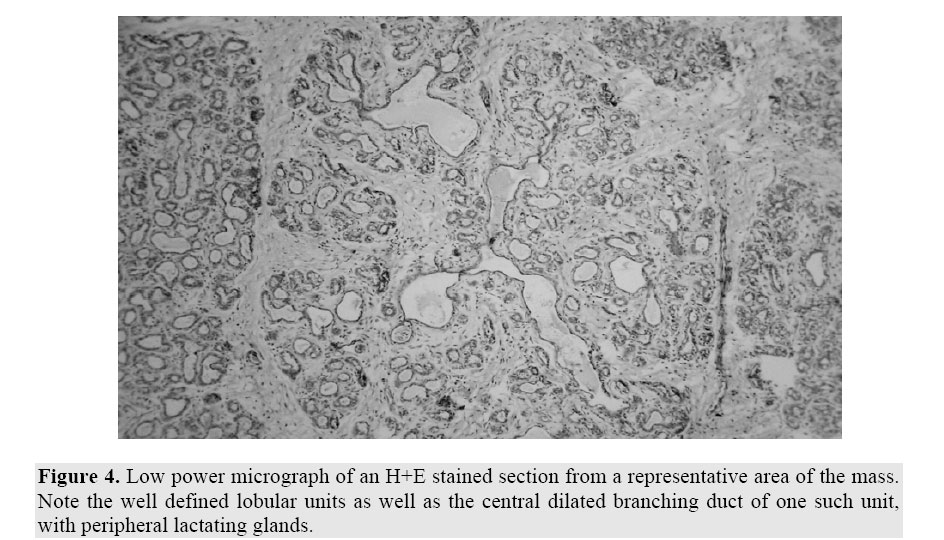
Lactating adenomas, more properly termed lactating nodules, occur in the pregnant and post partum patient and require investigation to rule out the possibility of a malignancy. Most often the clinical and cytological assessment suggest a benign process, however occasionally there is a suspicion of malignancy that requires surgical intervention, in order to both establish the correct diagnosis and remove the lesion. We describe such a case in order to sensitize physicians to this diagnostic challenge. Case Report At first presentation this G5 P4 22 year old living in rural western Uganda, first noted a mass in the upper lateral left chest during the seventh month of her pregnancy. A physical examination performed at that time by a physician documented a “small” mass in the left anterior axillary line, thought clinically to be benign. Over the next 5 months the mass grew rapidly, including the 3 month post partum period, when the mass ulcerated. She did not seek medical care during that time. When she became aware that a team of volunteer physicians (surgeons and pathologists) had arrived in her region, she sought further assessment and treatment. There was no history of breast carcinoma in the family. Her previous four pregnancies had been uneventful, with no breast masses noted. She had been breast feeding her newborn infant since delivery. There was no history of other illnesses. The patient was anxious, but vital signs were unremarkable, with no evidence of fever. The patient had two normally formed breasts, with another pendulous mass in the left axilla (Fig. 1). It measured about 20 cm in length with the last 5 cm towards the tip tapering more than the proximal mass. It was firm, with clinical delimitations proximally. The proximal surface toward the axilla was normal but with markedly enlarged venous drainage, developing a “peau d’orange” appearance towards the tip and ending in an ulcer. There was no nipple at the tip, nor elsewhere in the mass. The ulcer was round with raised edges and an uneven floor that was covered with necrotic tissue. The draining axillary lymph nodes were palpably enlarged. The left breast was considerably smaller than both the mass and the contralateral right breast. A well defined, 2 cm, non-tender nodule was noted in the upper outer quadrant of the left breast. The right breast was enlarged, showed a “peau d’orange”change, cutaneous edema and warmth, but was non-tender. A 6 cm well delimited, mobile mass was noted centrally. There were no palpable masses in the right axilla. The clinical features suggested inflammatory breast carcinoma with skin ulceration, involving ectopic left axillary breast tissue. The two other breast nodules were considered probably benign. Neither mammography nor ultrasound study was done. The patient was referred to the FNAC clinic. A pathologist (one of the authors) performed a fine needle aspirate of the ulcerated mass, its apical axillary extension, the left breast nodule, and the right breast mass. The cytological features of the ulcerated mass and its apical extension were similar and characterized by hypercellularity, discohesion and mild atypia, leading in the clinical context to a cytological diagnosis of carcinoma with axillary lymph node metastasis, probably arising in ectopic breast tissue (Fig. 2). The cytology of the left breast nodule suggested benign lactational change (not shown). The cytology of the right breast mass suggested a large fibroadenoma with lactational change (not shown), however a surgical biopsy was suggested to rule out malignancy. The ulcerated mass was resected, with removal of attached axillary nodes. Within the specimen there was a 22 cm X 13 cm ulcerated but macroscopically benign, circumscribed and lobulated mass, with a yellow-white cut surface (Fig. 3). The mass extended into the contiguous excised axillary tissue, which also contained enlarged but benign lymph nodes. The clinically noted masses in the two breasts were not sampled or removed. Histopathologic findings included enlarged ductlobular units with marked secretory changes and minimal stroma (Fig. 4), associated with an active chronic inflammatory process, including lymphocytes, eosinophils and plasma cells. At the site of skin ulceration there was only granulation tissue overlying the hypersecretory enlarged lobules. There was no evidence of malignancy or lymph node metastasis. The microscopic features were those of a giant but benign lactating adenoma with secondary skin ulceration. Discussion: Clinically, a lactating adenoma is not an uncommon breast tumour characterized by the appearance, during pregnancy or in the postpartum period, of a well defined, mobile, nontender breast nodule1. There may be a history of rapid growth2. The differential diagnosis includes other benign breast lesions such as cyst, fibroadenoma, galactocele and abscess, as well as phyllodes tumour and breast carcinoma. Fine needle aspiration cytology interpretation of breast masses in pregnant women is notoriously difficult due to the hypercellularity, cell discohesion and at least some nuclear atypia, potentially resulting in a false positive diagnosis3, as in this patient. Histopathologically, a lactating adenoma of the breast is a benign tumour characterized by a well circumscribed proliferation of benign duct-lobular units showing lactational changes, with variable background features, depending on the existence of an underlying lesion (for example an underlying fibroadenoma). There may be accompanying active chronic inflammation and sometimes areas of infarction as well1,4. Skin ulceration however has not been described before. The origin of lactating adenomas is debated. Possibilities include “de novo” neoplasms arising during pregnancy or the postpartum period, lactational change in pre-existing tubular adenomas or fibroadenomas, as well as lactational change in pre-existing areas of lobular hyperplasia. For these reasons it has been suggested that a better term might be “lactating nodule”, noting any underlying lesions, rather than “lactating adenoma”, which suggests a neoplasm1. Our case is one of the largest lactating nodules reported, measuring 22 cm X 12 cm. They usually range from 2-4 cm in size, but an enormous lactating nodule, similar to our case, has been reported once before2. That case also caused clinical concern with respect to inflammatory breast carcinoma, and histopathologic study of the resected mass was required to resolve the issue. It has only once before been reported in an ectopic location, but not with ulceration as in our patient 4. Nevertheless the ectopic location added to the difficulties in the interpretation of the fine needle aspiration cytology. This is the first report of a lactating nodule of the breast or ectopic breast in an African woman (a PubMed search using the term “lactating adenoma Africa” failed to produce any article). However one experienced general surgeon working in the Kampala-Jinja area of Uganda has on rare occasions seen clinically similar, although not ulcerated, lesions (personal communication). These also caused concern regarding malignancy due to their rapid growth rate. According to the surgeon however, they also proved to be benign after resection and microscopic study. Conclusion In summary this is a case report documenting the exceptional occurrence of a giant, rapidly growing but benign lactating nodule, with secondary skin ulceration, involving ectopic breast in a lactating Ugandan woman. It proved to be a diagnostic challenge pre-operatively, suggesting malignancy both clinically and cytologically, and required macroscopic study of the excised specimen as well as histopathologic study to establish its true benign nature. This experience suggests that clinically alarming breast masses in pregnant or lactating women should be approached with caution and no assumption be made about their nature, until a careful histopathologic study has established an accurate diagnosis. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06012f4.jpg] [js06012f3.jpg] [js06012f2.jpg] [js06012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}