 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 65-66 Hypernatremic Dehydration, Malaria and Septicaemia Complicated By Peripheral Gangrene In InfancyHelder de Miranda, Nutan Singhal.
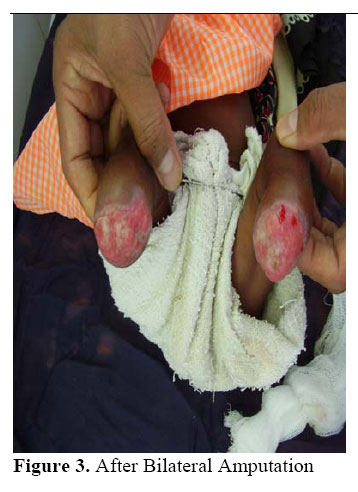
Department of Surgery, Beira Central Hospital, Moçambique Code Number: js06014 Introduction Symmetrical peripheral gangrene (SPG) is a rare clinical condition which manifest as ischaemic damage in two or more extremities without any evidence of obstruction or vasculitis of the relevant artery1. In infant this condition has been described in association with multitude of medical conditions among them being hypernatremic dehydration (HD)2,3, Falciparum malaria (FM)4,5, septicaemia, infants of poor control diabetic mother6. We report a case of symmetrical peripheral gangrene as rare manifestation of HD and FM. Case report A 53 days old female infant was referred to us from Dondo district hospital where she had been admitted with a history of fever, diarrhoea and vomiting. During her 6-days stay there, she had investigation for malaria that came back positive for plasmodium Falciparum. Treatment was started with i.v. Quinine. Despite the treatment, the child’s condition deteriorated. Both her lower limbs were noted to have turned blue. Two days later, the patient was transferred to Beira Central Hospital. On admission to Beira Central Hospital, the infant was found to be in a critical state with high fever and bilaterally gangrenous lower limbs up to mid leg level. On further investigation she had a haemoglobin of 6.2G/dl, RBC of 2.51, WBC of 26.200, neutrophil 63%, Lymphocytes 35%, Monocytes 2%, PLT 113.000, Na+ 170mmol/l, AST 104 ALT102, Total Protein 38, Albumin 18. HIV serology was negative. Chest X-ray was normal. The blood culture was sterile. She was started on treatment with i.v. fluids, antibiotics Ampicillin and Gentamycin and i.v. Quinine. After 3 days of treatment, she showed improvement in her general condition. The laboratory investigation returned to normal but the limb progressed to gangrene. A decision was made to perform bilateral below knee amputation. [Figure 1] [Figure 2] [Figure 3] Discussion Symmetrical peripheral gangrene (SPG) has been reported in a multitude of medical conditions including hypernatremic dehydration (HD), Falciparum malaria (FM) and septicaemia. According to available literature, HD causes hypoperfusion and sluggish blood movement due to hyperviscosity of blood, resulting in a disturbed microcirculation4,5. In the absence of convincing clinical and laboratory evidence of vasculitis or coagulopathy it seems likely that host factors (dehydration, sluggish peripheral circulation, platelet activation, subclinical intravascular coagulation) combined with strain-specific parasite factors (tissue sequestration of mature forms, rosette formation) may predispose to peripheral micro-vascular occlusion sufficient to produce infarction of tissue in susceptible children2,7. Pneumoccocal septicaemia is associated with intravascular coagulation and salmonella typhi infection is associated with vasculitis, both can cause SPG8,9. The baby improved very well after treatment with intravenous quinine, antibiotics and correction of HD, but unfortunately developed bilateral gangrene which resulted in bilateral below knee amputation. This would explain that the association of HD, FM causes SPG although it is a rare condition. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06014f1.jpg] [js06014f2.jpg] [js06014f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}