 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 75-80 Posterior instrumentation for spinal injuries and non-traumatic disorders. Report on surgical practice.Aldar Borissov1, MD (Orth.), Konstantin Borissov2, MD (Orth.) 1Mbuya General Military hospital; Kampala, Uganda. 2Orthopaedic
department, Mulago hospital. Kampala, Uganda. Code Number: js06018 Background: The purpose of the report is to show potential of the operative treatment with instrumentation for correction of traumatic and non-traumatic spinal deformities. Introduction Indications for operative treatment for spinal disorders are still controversial. The choice depends on anatomical and biomechanical peculiarities of different parts of the spinal column. Cervical spine is the area most often exposed to trauma and degeneration and early decompression is of the greatest value. The rib cage provides additional rigidity to the thoracic spine, at the same time making reduction of the deformities more difficult. Thoraco-lumbar spine fractures are very often unstable and require open reduction / internal fixation. Chronic degenerative conditions of the lumbar spine may cause severe disability to be treated operatively1. Operative treatment via Posterior Approach (PA) is one of the basic methods of spinal trauma and degenerative pathology care. The main advantage of PA is the possibility for wide exposure and revision of the vertebral canal and spinal cord. But wide laminectomy may destabilize the vertebral column. Limited approach to the anterior column (body and disc) precludes complete decompression and reduction of kyphosis. Modern techniques, including Internal Fixation offer a wide range of methods that overcome such difficulties. The aim of this study was to evaluate the early results of the operative treatment facilitated with internal fixation for various spinal disorders and the potential of the internal Fixators for correction of traumatic and non-traumatic spinal deformities. Patients and Methods A total of 95 patients with spinal disorders were operated on between 2001 and 2005. In 50 of them internal fixation via Posterior Approach was done. The age of the patients ranged from 2 to 66 years. X-rays were the main diagnostic method used to reach the diagnosis. Myelography and CT scan were done in 6 and 10 patients respectively. The distribution of disorders was as follows:
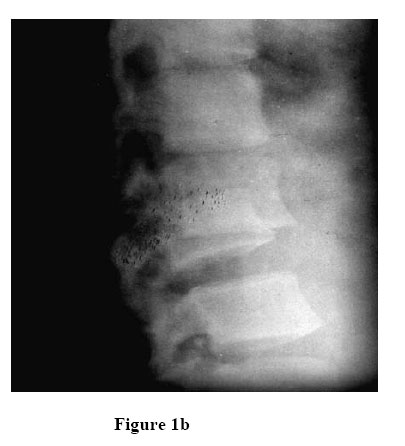
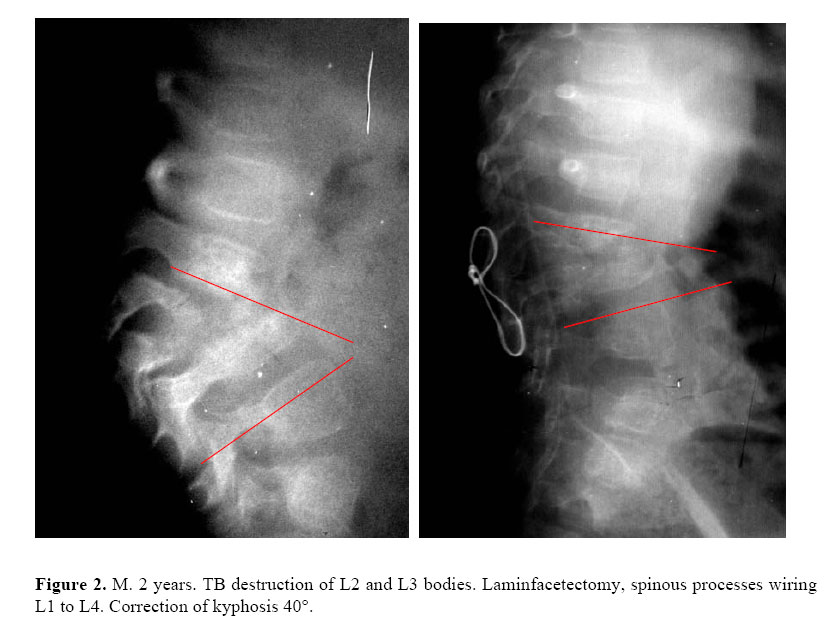
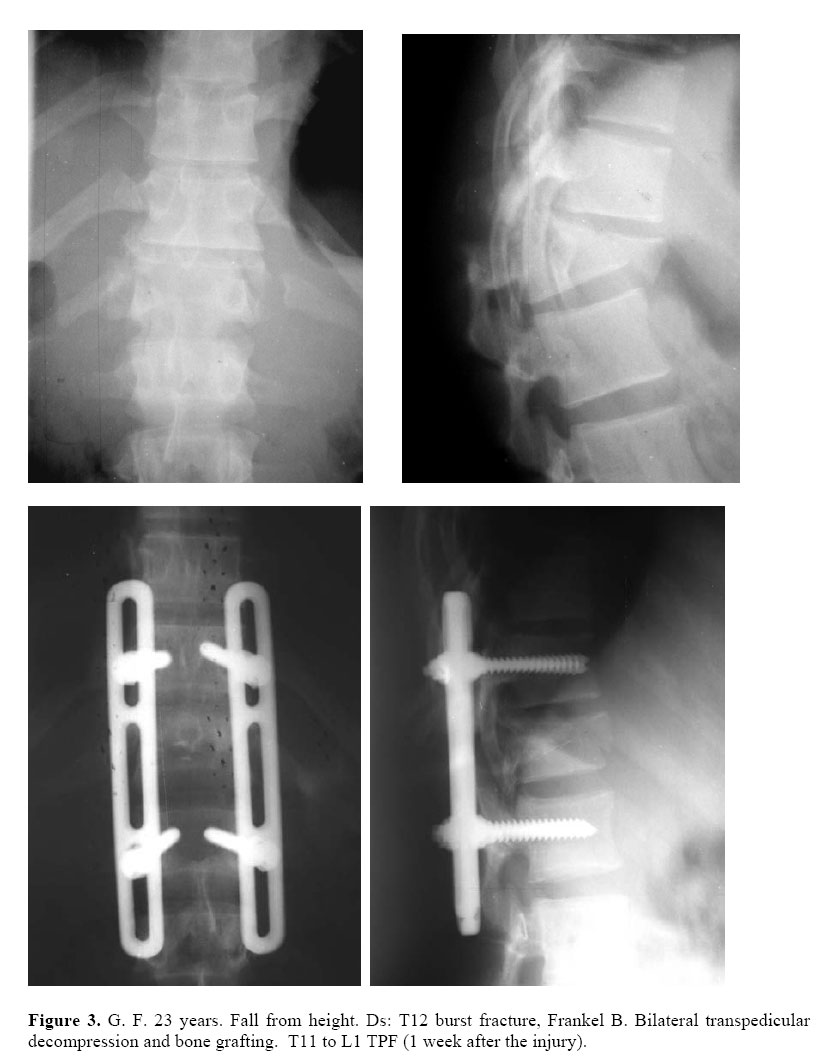
Forty patients had neurological deficit before operation. According to Frankel (1969), complete paraplegia was found in 12 of them (Group A), 8 had some sensory function preserved (Group B), 9 had paraparesis (Group C), and 11 were with some functional muscles below the injury (Group D). Instrumentation via PA was used to improve reduction of the deformity and rigidity of fixation. Fixation with soft wires was done in 10 cases (7 cervical spine, and 3 thoracic/lumbar). Spinous processes of 2 to 3 levels were engaged in order to achieve stability. In one patient screws were inserted into the lateral masses of the C5-C6. Transpedicular fixation (TPF) was used in 40 patients: Steffee system – 30, AO (Synthes) – 3, improvised fixation (with DCP plates) – 4, and external transpedicular fixation in 1. (Figure 1a and 1b). 2 to 4 segments were fixed depending on degree of instability. At the thoracic and lumbar levels, bilateral postero-lateral approach to the vertebral bodies was necessary to reduce old fracture-dislocation (5 cases). Anterior decompression in patients with burst fractures was done via pedicles, bilaterally (5 cases). method of stabilizing degenerated lumbar segments. In 1 case of degenerative scoliosis 3 segments were fused. Decompression was done in 3 of the 7 patients due to significant vertebral canal stenosis. ResultsWe performed revision of the spinal cord in 7 patients with neurological deficit. In 3 cases of TB spondylitis reduction of the deformity was done by *shortening* of the spinal column: removal of posterior elements (laminfacetectomy) of involved vertebras and fixation of the adjacent vertebras. Radiographic evaluation of surgery outcome was done (Figure 1a, 1b, 2, and 3). Total reduction of the deformity was achieved in all the cases of fracture-dislocation. Complete anterior decompression was achieved in all the patients with burst fractures. In patients with TB spondylitis, reduction of kyphosis was significant (from 80° to 30°) after posterior intervention with laminfacetectomy and instrumentation (Fig. 2). Solid fusion was obvious after 3 – 6 month in 4 of 7 patients with degenerative pathology of the lumbar spine. Clinical Results. Twelve patients with Grade A tetra/paraplegia did not gain any neurological function. Of 9 with Grade B, 4 improved to C and D. Of the 8 patients with grade C, 5 improved to grade D in 2-3 months. Eight of the 11 patients with grade D improved to Grade E the other 3 improved, but not enough to change the group. Neurological deficit increased postoperatively in two patients. Low back pain resolved completely in 5 of 7 patients with degenerative lumbar spine. Complications
Intraoperative complications Dural sac injury occurred in two patients. Liquorrhea developed in one patient with complete traumatic rupture of the dural sac. The sinus gradually closed in 3 months. Three patients died of pneumonia, UTI and sepsis during the early postoperative period. Bedsores developed in six patients. There were no cases of post-operative wound infection. Five screws were found broken in four patients after 6 – 12 months. Loss of reduction was critical in two cases where soft wires were used. Discussion In case of spinal injury all the efforts are directed towards restoring anatomical shape of the vertebral canal to create the best conditions for restoration of the neurological function. Complete reduction of deformity also prevents secondary loss of correction. Approach via PA makes it possible to correct the kyphosis by compression (compressors are more stable than distractors). On the other hand, anterior decompression (intervening vertebral body and disc) is often difficult, that is why bilateral transpedicular approach is useful2 (Figure 3). Implants designed 30-50 years ago for fixation of vertebral segments were not enough rigid and late loss of correction was common In the treatment of TB spondylitis anterior approach and grafting is the method of choice. But anterior fusion without fixation has low potential for reduction of the kyphosis. Even after long period of immobilization deformity may increase7. Certain patients are eligible for postero-lateral approach and instrumentation. Temporary increase of the neurological deficit after operation is common. It may be explained by severe stress to blood supply and mechanical irritation of the neural elements. That is why surgical intervention must be maximally gentle. Patients of Frankel A group usually do not gain any neurological improvement (possibility is less then 3%). Most of the patients with incomplete injury improve up to next group, at least8. Pneumonia and resultant ventilatory failure is one of the main causes of early death after severe spinal cord injury. Early mobilization facilitated by operative stabilization is the main prophylactic measure of such complications9. Liquorrhea is almost inevitable in vast dural tears but usually subsides in 2-3 months. The management consists of mechanical pressure, medical suppression of the liquor production and repeated tapping. Infection of the operative wound is rare complication due to the rich blood supply of the spinal muscles. In degenerative pathology careful selection of patients is crucial10. Short-segmented fixation may spare healthy mobile segments. Rigid fixation facilitates the rate of fusion11. Conclusion
Every patient is to get differential approach depending on type, localization of the disorder and neurological status. Variants of posterior approaches are indicated in burst fractures, degenerative disorders and especially in fracture-dislocations of any localization. Also, if a patient has got smaller sizes of the trunk, there are more additional indications for PA. Spinous processes wiring is reasonably adequate method to stabilize cervical spine fracture– dislocations, but very often we found them to be broken, or too tiny to obtain reliable fixation. In these cases, lateral mass screwing and plating should be utilized more often. It is more stable, does not require intact lamina or spinous processes. Sometimes, this may shorten the overall fusion length12. Transpedicular fixation is the method of choice in fracture-dislocations of thoracic and lumbar spine. Superior reposition and rigid fixation can provide best conditions for rehabilitation of patients with severe neurological deficit13. In burst fractures of the thoraco-lumbar spine TPF allows restoration of the physiologic curvatures and rigid fixation. Decompression can be achieved via bilateral transpedicular approach. In order to overcome the disadvantages of PA we recommend: complete decompression of lumbar burst fractures via bilateral transpedicular or posterolateral approach, reduction of kyphotic deformity by compression rather than by distraction. Multilevel fixation may be avoided by using short and rigid transpedicular systems. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06018f1b.jpg] [js06018f1a.jpg] [js06018f3.jpg] [js06018f1cd.jpg] [js06018f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}