 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 81-86 Breast Cancer in an Ethiopian Population, Addis Ababa Tessema Ersumo, MD, FCS-ECSA
Associate professor of surgery, Tikur Anbessa Hospital Department of Surgery, P. O. Box 9086, e-mail: naat@ethionet.et Tel No. 251 9 20 97 98, Addis Ababa, Ethiopia Code Number: js06019 Background: Breast cancer is a major life-threatening public health problem of great concern. Long-term increases in the incidence of the disease are being observed in both industrialized and developing world. Introduction
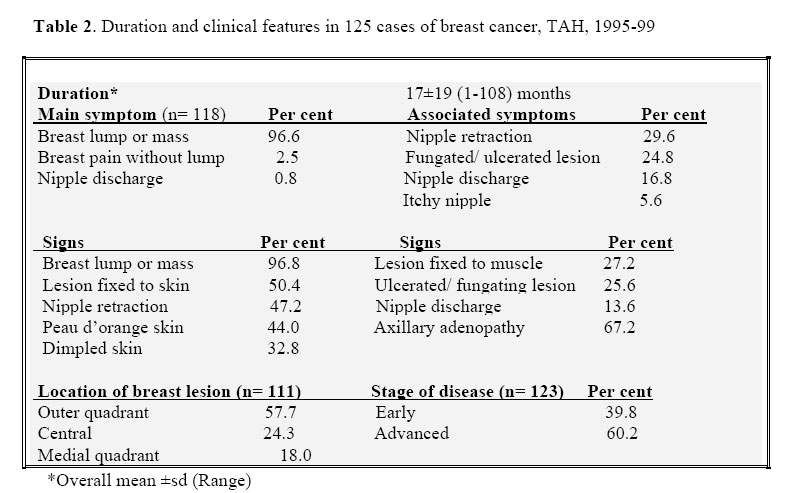
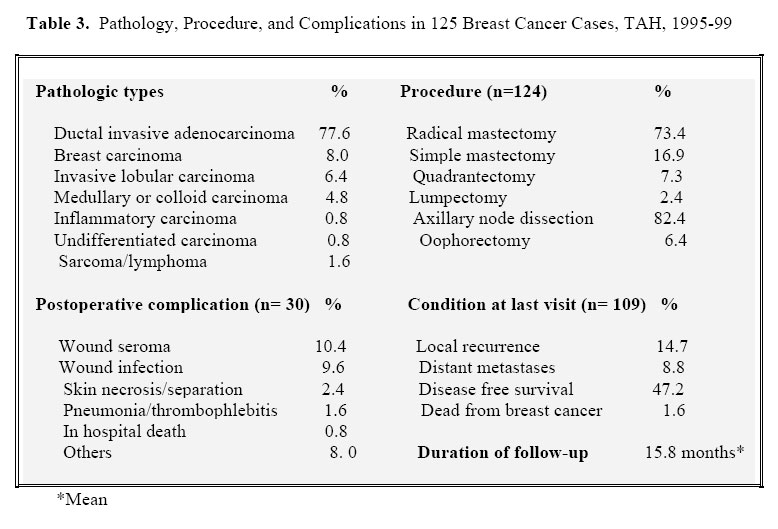
Breast cancer is a major public health problem of great importance1. It is a stressful disease to those affected2. Worldwide, increase in the incidences of breast cancer is being observed3. The increase is considerable below the age of 50 years. After menopause, the incidence rates continue to rise, but less dramatically1. In general, in the less affluent and third world countries, the same but much lower pattern of increase with age is seen4-6. Diagnostic delays of 3-6 months are associated with advanced stage breast cancer and lower survival. Detection and treatment of cancer at an early stage improves the prospects for long-term survival7. In Ethiopia, there is no cancer registry and the incidence of the disease is unknown. The aim of this retrospective study was to analyze the pattern and treatment outcome of breast cancer in a teaching hospital. Patients and Methods In the years 1995 to 1999, 137 histologically confirmed breast cancer patients underwent surgery at Tikur Anbessa Hospital (TAH), Addis Ababa. Of these, the records of 125 cases were retrieved and analyzed. TAH is a central tertiary referral hospital with adult surgical bed capacity of about 200. Information obtained from the records of patients included demographic characteristics, clinical and pathological description of cancer, treatment and outcome. Diagnosis of metastases was based on clinical evaluation, cytohistological examination, or radiological studies. TNM8 crude stage of the disease was based on information stated in patients’ records. During the years under review, TAH had no established breast cancer treatment protocol and hence decision on the type of surgical procedure was made mainly by the individual surgeon. Breast conserving therapy (BCT) with axillary node dissection, most probably due to patient preference, was offered in only 12 patients; 11 of them had stage II disease. One patient with stage IIIb disease also underwent quadrantectomy because of refusal to undergo mastectomy. Modified radical mastectomy with axillary node dissection was performed in patients with stage I and II. Toilet mastectomy was performed for mobile ulcerated fungating tumours with or without distant metastases. Postoperatively, ipsilateral chest or axillary subcutaneous or skin nodule verified as breast carcinoma was termed as local recurrence. Data were collected on a pre format and entered into a computer. Data analysis was performed using Epi info version 6 software and relevant statistical analysis was done using the available statistical package. Results The majority (55.2%) of the patients were in the 30-49 age group. Only 5% were 25 years old or below (Table 1 and Fig. 1). The age for females ranged between 20 and 80 years with a mean of 42.4±11.9. In males the ages ranged from 37 to 80 years with a median 55.8±13.3. Out of 112 females, 13.4% and 70.5% were under the age of 30 and 50 years, respectively. Most patients were premenopausal women. The median parity was 4±2 but 18.1% were young nulliparous women. Majority of cases were Amhara by ethnicity and Christian. The median duration of the presenting symptom on admission was 11.5±19.3 months (Table 2). Of 118 patients with documented chief complaints, 92.4% had initially painless breast lump. Breast pain without lump or nipple discharge as the main presenting feature was rare. About 50% of cases had locally advanced lesion and a quarter presented with ulcerated or fungating lesions. History of pregnancy or lactation was documented in 103 cases; 12 were pregnant or lactating at or after the detection of breast lesion and 3 became pregnant during breast cancer treatment; 8 of these had stage III disease. History of benign breast disease (6%), contralateral breast (3%) or non-breast cancer was rare. The most common signs were breast mass and axillary metastasis. Sixty-seven (54%) patients had mobile and 20(16%) fixed ipsilateral axillary lymph nodes. The location of lesions was specified in 111 cases; 49% were in the upper outer quadrant. Sixty per cent (n= 118) of cases had tumors larger than 5 cm in diameter. Lesions fixed to the underlying muscles (34 cases), mainly the pectoral muscles, were not rare. Twelve (10%) patients had distant metastases, 6 in the lung, 5 in bone, and 4 in the liver. Clinically, majority of cases (60.2%) had stage III and IV disease, in nearly all locally advanced stage III disease. Satellite skin nodules (7%), supraclavicular (6%) or contra lateral axillary (2%) node metastases were rare. No case of Stage I disease was not recorded. Ductal invasive adenocarcinoma was the most frequently (77.6%) reported pathological type (Table 3). Other rare lesions included colloid/mucoid, comedo, papillary, or squamous cell carcinoma, lymphoma, and sarcoma (1 each). Eighty-nine patients (71.8%) underwent modified radical mastectomy and 103, axillary dissections. In 21 patients, toilet mastectomy was performed for ulcerative/fungating tumors. Only 12 cases underwent breast-conserving surgery with axillary dissection, 9 quadrantectomy. Fortytwo patients received combined or single adjuvant therapy including radiotherapy (29), chemotherapy (20), tamoxifen (19), and or oophorectomy (8 patients).Out of 10 BCT cases that received adjuvant therapy only 6 had radiotherapy. Follow-up was possible in 109 cases (87.9%) for a median duration of 10 months. Of these, 58.7% had follow-up for 1 year or less, only 4 for 5 years or more. Fifty patients (45.9%) were seen with recurrences (46 females); 16 (32%) had local, 11 (22%) distant, and 21 (42%) had both local and distant recurrences. All the recurrences were following toilet (12cases) or radical mastectomy (38 cases) with or without adjuvant therapy. The most frequent sites of recurrence or metastasis were the skin (28), ipsilateral axilla (17), lung (17) and bone (10 cases). Two (4%) died from the disease. Condition of 15 (12%) was unknown; 11 had stage IIIB or IV disease. During a mean followup time of 2 years, all 12 BCT cases were seen with no evidence of local or distant recurrence. Short-term clinical disease-free or improved survival was observed in cases of stage II disease regardless of age and in those that received multimodality therapy. Discussion Breast cancer development increases with age, beginning to rise at approximately age 30 years2. In this study, 13.4% of cases were under 30 years of age. Most breast cancers occur during the postmenopausal years. Among Japanese women, however, no postmenopausal incidence risk occurs; it is puzzling6. In our series as well, in conformity also with other African experiences9,10, most women with breast cancer were in the premenopausal state, about 70% less than 50 years of age. In the US, nearly 85% of women with newly diagnosed breast cancer have disease that is clinically limited to the breast or regional nodes11. In this series, the median duration of the presenting symptom at admission was 11.5 months and 60% of 118 cases had tumors larger than 5 cm in diameter, findings similar to those of African series9,10,12 disclosing excessive late presentation and advanced stage of the disease. Carter et al13 reported nodal metastases at diagnosis of around 40%; this was 67.2% in our series. Globally and in this series as well, in both sexes and all ages, infiltrative ductal and lobular breast carcinomas are the most common histological types accounting for 61-80% and 510% of cases, respectively2,14-17. Breast carcinoma in men accounts for 0.5% of all breast cancers in the United States (18) and 2.4% to 15% in African series19, 10.4% in the present study. The reported median age of breast cancer in men varies from 56 to 59.6 years 14,20, 55 years in this series. The treatment of male and female breast cancer are similar14. Detection and excision of the primary tumor at an early stage improves the prospects for long-term survival7. In women with clinically positive axillary nodes, modified radical mastectomy and axillary dissection are excellent to achieve and maintain local control of breast cancer obviating radiation therapy2,21. For breast conserving surgery (BCT) to be successful, the tumor must be small confined to a quadrant and the patient must undergo radiotherapy11,17. Few cases underwent BCT in this series. As was also observed in 8 of 12 patients in this study, pregnant patients have more advanced stage cancer and radio- or chemotherapy is risky before 30 weeks of gestation. Modified radical mastectomy without delay is the best option in pregnant women with stage I to III cancer22. The primary goal of treatment of metastatic breast cancer remains palliation of symptoms and improvement of the quality of life23. Effective control of locally advanced or recurrent disease, as was routinely attempted for the former in our series, is important because uncontrolled local disease significantly impairs the quality of life causing ulcerations, bleeding, foul discharge, debilitating limb edema and pain24. Recurrence of breast cancer is psychologically devastating indication of therapeutic failure 25,26. An overall locoregional relapse rate of between 5% and 30% has been reported26 with a palpable mass appreciable in 70 to 90% of cases27. Numerous surgical studies show that the risk of locoregional failure is directly proportional to the extent of axillary lymph node involvement and the size of primary tumor21,28-31. Most locoregional relapses develop in the skin of the chest, a harbinger of distant metastases23,26,28. Following axillary dissections, axillary nodal recurrences are rare29; 34% axillary relapse rate in our series was probably due to an initial advanced disease. In this study, during a short postoperative follow-up, 50 of 109 cases developed local or distant recurrences. As cited by Zavosteky and Gardner, several studies have found that 88 to 94% of recurrences are at or near the primary site32, 74% in this series. This study is limited by its retrospective design, lack of cancer registry and the relatively small number of cases. However, it appears that breast cancer affects young age group and majority present late. General guiding principles of breast cancer therapy are early detection and aggressive local treatment to prolong survival. In healthcare facilities where timely commencement of adjuvant therapy is restricted or where the therapy is unaffordable or inaccessible, mastectomy should be the initial option. Effective control of locally advanced or recurrent disease may improve quality of life of a patient and should be attempted in selected cases. Public awareness of the disease to identify patients with localized disease is important in the pursuit to cure breast cancer. Patients with symptoms that could be due to breast cancer should be referred without delay for specialist assessment. To uncover the magnitude of the disease in Ethiopia and to produce national breast cancer treatment guidelines a collaborative multicenter study is desirable. Cancer registry should also be introduced. Acknowledgement The medical records unit of Tikur Anbessa Hospital cooperated in patient chart retrieval. Grateful thanks are also due to all who participated in the care of the patients. Ato Kidane Mariam Woldeyesus, Addis Ababa University Faculty of Medicine, assisted in data entry and statistical analysis. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06019t1.jpg] [js06019t3.jpg] [js06019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}