 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 87-93 Preliminary Results on Polypropylene Mesh Use for Abdominal Incisional Hernia Repairs: The Experience at KCMC – Moshi, Tanzania; 2001 –2005. Samwel Chugulu, Abduel Kihunrwa Code Number: js06020Background: Incisional hernia is a major surgical problem. Several methods
of hernia repair have been described but their outcome has been disappointing.
This preliminary retrospective study reports on our experience with
polypropylene mesh repair. Introduction
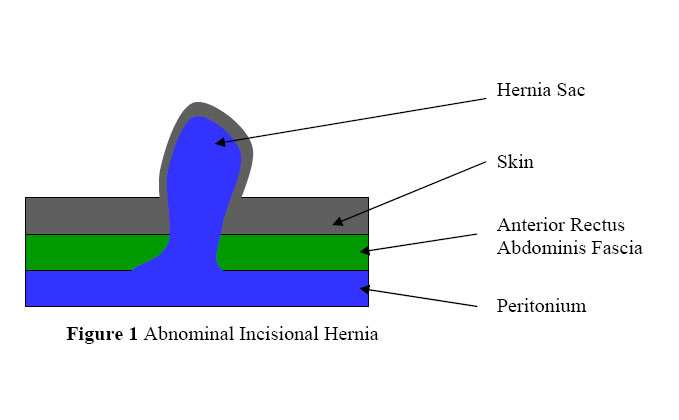
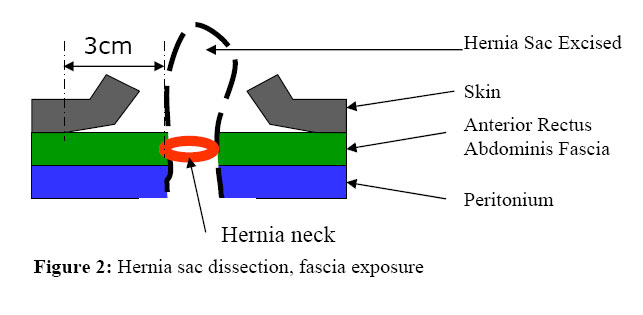
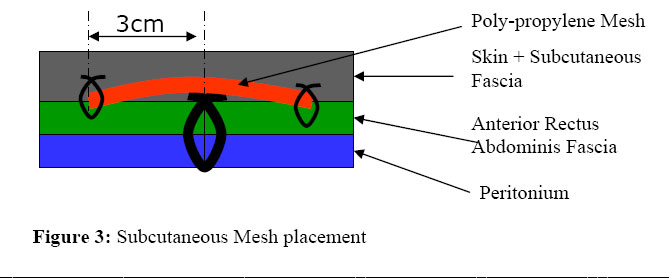
Incisional hernia is a major health care problem. It is one of the most frequent long term complications of abdominal surgeries. Incisional hernias appear in at least 10% of patients with laparatomies1. Numerous endogenous and exogenous factors are believed to play a role in the genesis of primary and recurrent incisional hernias. In the exceptional case, a single cause may exist, but more often the causes are numerous, complex and interrelated.2,3,4 Hernias occurring during the early post operative days should probably be largely attributed to technical failures, likely loosening of knots, breaking of sutures, or suture cutting through tissues; mostly brought about by high (intermittent) intraabdominal pressure. Here, the genesis of post operative herniation is similar to that of wound disruption3. Late hernias are more likely to be due to complications endogenous wound healing and constitution3. In long term follow up studies, its demonstrated that the incidence may be expected to almost double after the first year.5 Ninety percent of incisional hernias occur within the 3 years of operation6. Most incisional hernias are symptom-free and are discovered only upon routine physical examination. However, incisional hernias can be a significant source of morbidity and delay in repair may have serious clinical consequences6. Facial defects especially the small ones, predispose to incarceration in 6 – 14.6% and strangulation in 2.4% primarily of small bowel3,7,8,9,10. Hernias may increase in size with increasing difficulty of repair and higher recurrence rates11. Massive hernias may give rise to dystrophic ulceration of the skin, subsequent evisceration, difficulties in bending over, chronic abdominal pain, back pain and respiratory complications due to diaphragmatic dysfunction.12 Patients may have complaints about the esthetic appearance of their incisional hernia, ranging from a disfiguring lump and difficulties with clothing to feeling of inferiority13. Although many techniques of repair have been described, the results are often disappointing. Suture repair by various techniques have been practiced for ages. Here, one can opt for single layer or two layers or Mayo’s repair etc. The use of pedicle flaps is another option of hernia repairs. Pedicle fasciomyocutaneous extended lattissimus dosi flap, or fasciomyocutaneous tensor fascia lata flap or pedicle myocutaneous rectus femoris flap are examples. Among the problems related to flaps is the need to do an extensive surgery, functional deficits of the donor site and the repaired wall does not gain much strength. Pedicle flaps have therefore been preferred for recurrent infected mesh repaired hernias. Prosthetic mesh is either absorbable (eg. Polyglactin 910), or Non-absorbable (eg. Polypropylene, expanded polytetrafloroethylene - ePTFE, Polyster) Prosthetic repair have the added advantage of avoiding excessive tension and reinforcing the weakened abdominal wall by approximating the patients own tissues. However, prosthetic repairs have complications like visceral adhesions when the mesh comes into contact with the bowels. Also, the irritation can lead to paralytic ileus or even intestinal fistula formation. Polypropylene mesh has been the most preferred prosthetic due to its low infection potential and therefore performs well in the presence of infection. Following primary non-prosthetic repair, recurrence rates ranging from 24 to 54% have been reported8,14. Prosthetic repairs seem to have better but still high recurrence rates of up to 34%15 Following recurrent incisional hernia repairs, recurrence rates up to 48% have been described16. These preliminary results evaluate the 5 years experience on repairs of incisional hernias by the technique of placing the polypropylene mesh on the anterior rectus abdominis fascia done in the department of surgery, KCMC. Patients and Methods Records on patients with incisional hernias repaired by polypropylene mesh at KCMC main operating theatre from January 2001 to October 2005 were retrospectively reviewed. Patient related factors including age, sex, obesity, cough, diabetes mellitus, glucocorticoids use were recorded. The Body Mass Index (BMI) was calculated as weight (kg) / height (m2); obesity was defined as BMI > 30 Hernia related factors recorded included the site of hernia, whether supraumbilical, infraumbilical, and paraumbilical, size of hernia. Operation related factors noted were the type of previous surgery, type of abdominal incision, number of previous surgeries, numbers of previous hernia repairs, sac components and procedures done on the viscera. The prophylactic antibiotics used were recorded. After skin preparations and draping, the cutaneous scar was excised. This was followed by hernia sac dissection to expose the abdominal wall defect with a 3 cm circumferential margin of healthy fascia (Figures 1 and 2). The hernia sac was opened, inspected and reduced. Adhesions if present were released. Excision of the omentum was done if the patient was obese and the large omentum was suspected to have contributed to the raised intra abdominal pressure. Hernia sac was excised leaving margins for defect closure. Running vicryl, or prolene or nylon suture was applied along to close the abdomen. Polypropylene mesh of appropriate size was placed on the closed defect with about 3 cm of overlapping mesh over healthy fascia all around the defect. A running suture of polydioxanone (PDS®) or nylon or prolene was applied around the edges of the mesh on the healthy fascia. (Figure 3). In most of the patients, a subcutaneous tube drain was placed and exteriorized through a separate stab incision. Skin closure was finally done. Post operative complications and days of hospitalization were recorded. The indication for drain removal was when the 24 hours output was less than 20 cc. The most recent documented physical examination was used to determine hernia recurrence and follow up. Results
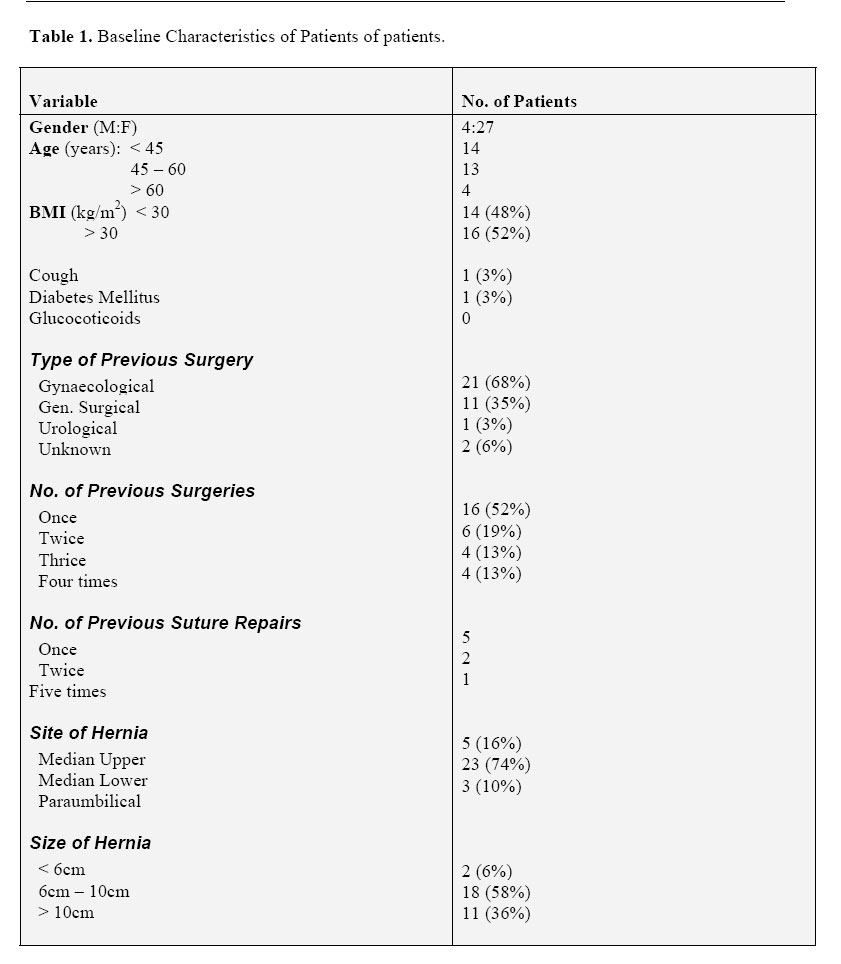
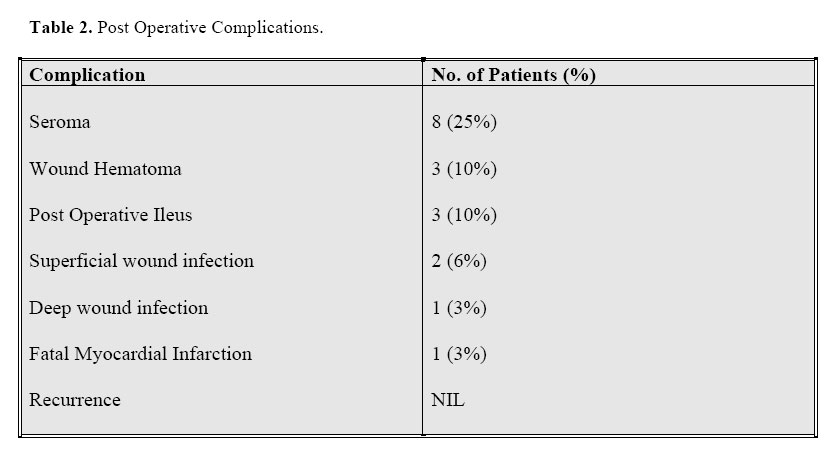
A series of 31 patients had polypropylene mesh repairs on abdominal incisional hernias during the study period. One patient died 2 hours post operatively due to cardiac arrest secondary to coronary arterial disease. No other mortality occurred in hospital. The resultant hospital mortality rate was 3%. The remaining group was comprised of 26 women (87%) and 4 men (13%) with a mean age of 47 and a range of 26 to 67 years. The Risk factors found to have contributed to raised intra abdominal pressure and impaired wound healing were as shown in Table 1. Previous history of gynaecological procedures contributed to the majority (68%) of incisional hernia case. About half of the patients had more than one previous abdominal surgery. Majority (74%) of repaired hernias were lower median positioned. Hernia sizes were in 94% larger than 6 cm in diameter. Prophylactic antibiotics were given to 27 (90%) of all patients; ceftriaxone in 18, cloxacillin – 3, ciprofloxacin – 2, ampiclox 2, gentamycin – 2, chloramphenical – 3 cases). Duration of post operative hospitalization varied from 2 to 27 days with a mean of 6 days. Postoperative follow up duration ranged from two weeks to 46 months with a mean of 15.4 months. Among the post operative complications, seromas developed in 8 cases (25%), 2 patients had superficial wound infection, 1 patient had a deep wound infection which necessitated mesh removal (Table 2). No hernia recurrence was recorded. Discussion The use of prosthetic repair is the method of choice for all non-emergency incisional hernia repairs, irrespective of size17. The 3 year cumulative recurrence rate of the suture and mesh repairs were 43% and 24% for primary repairs (p=0.02) and 58% and 20% for first time recurrent repairs (p=0.01)17. ‘Edge-to-edge’ hernia repair may lead to excessive tension and subsequent wound failure due to tissue ischaemia and sutures cutting through tissues18. On the other hand, the use of prosthetic mesh repair allows defects of any size to be repaired without tension. Polypropylene mesh, a non absorbable mono filament mesh, has been liberally used for decades. By inducing an inflammatory response, it sets up the scaffolding that, in turn, induces collagen synthesis. Furthermore, its superiority over other prosthetic mesh (polyster, expanded polytetrafluoroethylene – ePTFE) is seen by its low infection potential ability and therefore performs well in presence of infection19,20. At KCMC, out of the 31 cases with incisional hernias who had polypropylene mesh repairs, 52% of the patients were obese. Although the number of patients studied was not enough to draw statistically conclusive results, the findings help us to support the known fact that obesity is one of the risk factors of raised intraabdominal pressure and fatty infiltration decreases the quality of abdominal musculature3. It is also technically more difficult to approximate wound edges in a patient with a heavy pendulous abdomen. The thick layer of adipose tissue produces a distracting force on wound edges and preventing dead space is more difficult. Excision of omentum is recommended by some authors to facilitate closure19. Also, post operative wound infection is higher in obese patients. About 70% of incisional hernias were lower median located. Previous gynecological procedures contributed to about 70% of incisional hernia cases. This can be partly explained by the fact that probably a reasonably large number of emergency obstetric and gynaecological procedures in the periphery are done using poor surgical skills. There is a need to do a thorough evaluation on this matter. Irvin and Bucknall21 identified the surgeon’s experience as a risk factor for hernia occurrence. On comparing between upper, lower and complete midline incisions, most prospective studies do not show a significant difference in incisional hernia rate22,23. Regnaud et al24, however, in a prospective non-randomized study with up ten years of follow up, found a significant difference between fresh infra umbilical (16.6%) and supra umbilical (7.2%) midline incisions (p=0.001) The lack of posterior fascia below the Arcuate of Douglas, which usually lies 3-5 cm below the umbilicus may be responsible. Among the post operative complications, wound infection constitutes an undebateable risk factor for wound failure. Several authors consider wound infection to be the most important factor contributing to development of recurrent incisional hernia13,17,20,22,24,25. In our review, two patients had superficial wound infection which responded well to daily povidone-iodine and normal saline cleaning. Deep wound infection necessitating removal of the mesh was noted in one patient. Abramor et al showed that the single dose cephalosporin prophylaxis administered 30 minutes before incisional hernia repair significantly reduced wound infection rate. Mung’ong’ et al in KCMC, 2004 found an equal benefit against abdominal wound infection when chloramphenical was used as compared to ceftriaxone. Seroma (8%) and haematoma (3%) were among the post operative wound complications. The drainage of subcutaneous tissue through separate stab incisions has been done to most of the mesh repaired cases. This might lower the incidence of hernia recurrence as a result of secondary wound infection. George18 found that a significantly higher proportion of patients (p=0.0004) who had post operative wound complication (haematoma, wound infection or seroma) developed recurrent hernia. In our review, there was no single recorded case of hernia recurrence. However, our median follow up time was on average only 15.4 months compared to the recommended time of at least 36 months. Future Plans There is a need to prolong the follow-up time and increase the sample size so as to have statistically significant analyzable results. There is a need to conduct a study between suture repair on abdominal incisional hernias versus polypropylene mesh repair by the fascial on lay placement technique in the Tanzanian setup. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06020f3.jpg] [js06020t1.jpg] [js06020f1.jpg] [js06020f2.jpg] [js06020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}