 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 99-101 Acute Cholecystitis –Current Views A.M Gakwaya1, J Jombwe2 1Senior Consultant Surgeon,. 2Senior Registrar, Mulago Hospital, Correspondence to: AM Gakwaya, P.O. Box 7051, Kampala-Uganda, E-mail: gakwaya@utlonline.co.ug Code Number: js06022 Acute cholecystitis is predominantly a disease of females who account for 62 percent of cases and mainly affects those between 40 and 50 years1 and is closely associated with cholelithiasis. It occurs all over the world but Africa is a low risk area as compared to Europe and North America. The disease has been observed in children with ascariasis or those with acquired immune deficiency syndrome (AIDS). The commonest bacteria isolated in acute cholecystitis are E Coli. Clinical presentation includes a raised temperature. Leukocytosis may be absent even in those patients with gangrenous acute cholecystitis. However, Murphy's sign remains very specific. The mainstay of treatment remains surgical either open or laparoscopic cholecystectomy and in high-risk patients percutaneous or open cholecystostomy. Laparoscopic cholecystectomy has greatly increased operating time but reduced hospital stay. The over all mortality has remained 5-12% in the last 2 decades. Aetiopathology It is agreed that the disease goes through a definite chain of obstruction, chemical injury, inflammation and bacterial invasion. The commonest isolated bacteria are: E Coli 60%, Klebsiella, streptococcus and others2. A total of 95% of acute cholecystitis are associated with stones and 15% of gallbladders with stones develop acute cholecystitis. Other predisposing factors include old age, diabetes mellitus, typhoid fever, renal impairment, arteritis, polyarteritis nodosa3 and malignant hypertension. Five cases have been reported following Trucut liver biopsy and a few following gallbladder torsion4. Other associated problems include ductal stones in 20%, chronic pancreatitis in 7% and Cancer of the gall bladder in 1%. Bacteriology Csenders5 showed that when the common bile duct or gall bladder is aspirated the prevalence of positive bacterial cultures is 0% in normal people, 22% - 46% in patients with gall stones or acute cholecystitis and 58.2% in common bile duct stones without cholangitis or previous cholecystectomy. Similar bacteria were isolated from the gall bladder and common bile duct. Gender or number of stones did not influence the number of positive cultures but advancing age increased the positive cultures. Acalculous acute cholecystitis accounts for about 5%. The bile is lithogenic or sometimes the stone has already been passed. Acalculous acute cholecystitis is usually associated with major surgery, burns, fasting, general. anaesthesia, analgesics, dehydration, ileus, multiple transfusions, sepsis, ductal stenosis, choledochal cyst, diabetes mellitus, and old age. Sometimes stool may show some stones. Natural history of patients with acute cholecystitis Complete recovery following acute inflammation occurs in 75% recover completely and only 25% are met with complications which may even be fatal. Gangrene occurs about the third day in about 15%. Empyema occurs in 5% and it is more common in elderly male with diabetes mellitus. Perforation occurs in about 5%. The perforation may be into the local organs, it may form a peri-cholecystitis abscess or a patient may develop generalized peritonitis. Symptomatology The usual symptoms of pain 30-90 min after a meal, fever, nausea and vomiting may not be present in a number of patients (6). A palpable mass appears after 24 hour in a third of patients, toxicity, guarding, and jaundice indicate complications. Murphy's sign is not useful in elderly patients7,8 as illustrated below:
Treatment
The treatment is immediate cholecystectomy. On admission to hospital, a nasogastric tube (3mm) for gastric decompression is passed and intravenous fluids and antibiotics, (cefuroxime or mezlocillin) prescribed. Immediate cholecystectomy carries a mortality of 5-10 percent10. However there is a small percentage of patients who have other medical diseases which require to be stabilised first. Among these if life is threatened (impending gangrene or rupture) they are offered cholecystostomy and later when they have stabilised cholecystectomy is done. If life is not threatened the medical condition is stabilised and later cholecystectomy is done.
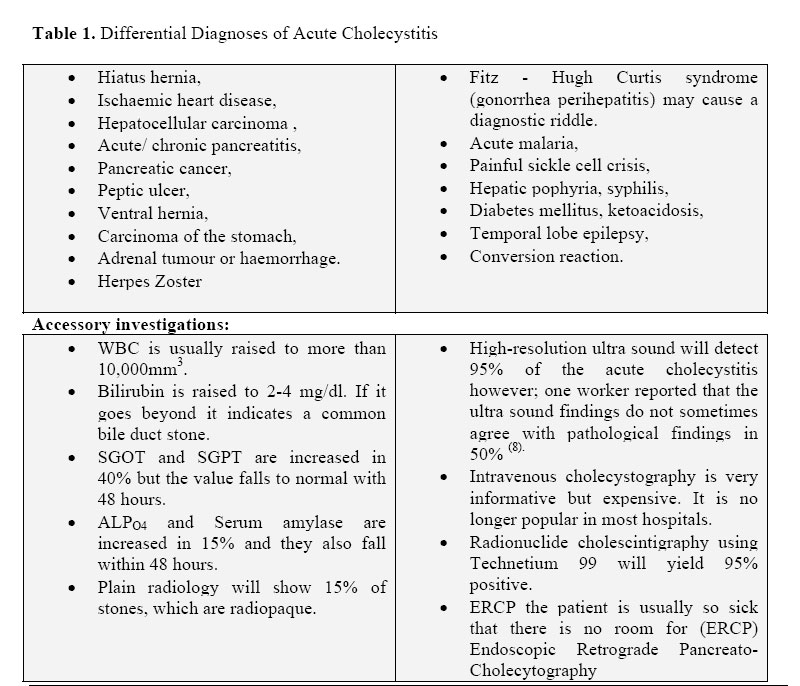
Differential diagnosis
Conditions to be considered in the differential diagnosis are shown in Table 1. However LC is contraindicated where there is an older scar or if one is suspecting adhesions. In terms of relative costs, percutaneous cholecystostomy costs US$ 1620, open cholecystectomy US$ 3155, while laparoscopic cholecystectomy costs US$ 5,000. However LC is contraindicated where there is an older scar or if one is suspecting adhesions. In terms of relative costs, percutaneous cholecystostomy costs US$ 1620, open cholecystectomy US$ 3155, while laparoscopic cholecystectomy costs US$ 5,000. Cholecystostomy This procedure is left for those who have other medical conditions, which are a contraindication to cholecystectomy, e.g. congestive cardiac failure. The purpose is to decompress the gall bladder in order to prevent gangrene and perforation. A cholecystectomy should be done as soon as the patient has stabilized. Cholecystostomy may be -open cholecystostomy. It has a mortality of 5-12 percent 11, 12, 13. Percutaneous cholecystostomy It may be transhepatic or transperitoneal. It has fewer complications than the open. Ultra sound guided Percutaneous Cholecystostomy (UGPC), Patterson10 did 43 and 90% improved within 48 hours. However the surgeon must be at hand for further treatment. Special cases: Indin14 reported 18 children with acute cholecystitis. They all had organic disorders of the gall bladder and cystic duct. Khuroo15 has described ascaris as a cause of acute cholecystitis in addition to other complications. Wittman16 has suggested that acute cholecystitis may occur in Acquired Immune Deficiency Syndrome (AIDS). Surgeons are advised to take extra care while handling these emergencies. Mortality Mortality increases with age and poor health but all in all is 5-12 percent10. The common causes of death are sepsis, pneumonia and cardiac complications. Conclusion Inspite of the development of new antibiotics, imaging and laparoscopy, the mortality of acute cholecystitis has remained 5-12% for the last two decades. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06022t1.jpg] |
| |||||||||

{kind=link}