 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 1, April, 2006, pp. 110-117 Bacterial Pathogens Associated with Tap and Well Waters in Lagos, Nigeria. Akinyemi KO1 , Oyefolu AOB 1, Salu OB2, Adewale OA1 and Fasure A K1. 1Department of Microbiology, Lagos State University, (LASU) Ojo, P.M. B, 1087, Apapa, Lagos, Nigeria.2Nigerian Institute of Medical Research, P.M.B. 2013, Lagos, Nigeria. Code Number: js06025 Background: The increasing cases of waterborne diseases in recent times necessitated the investigation of well and tap waters, which serve as source of drinking water in Lagos, Nigeria. Introduction
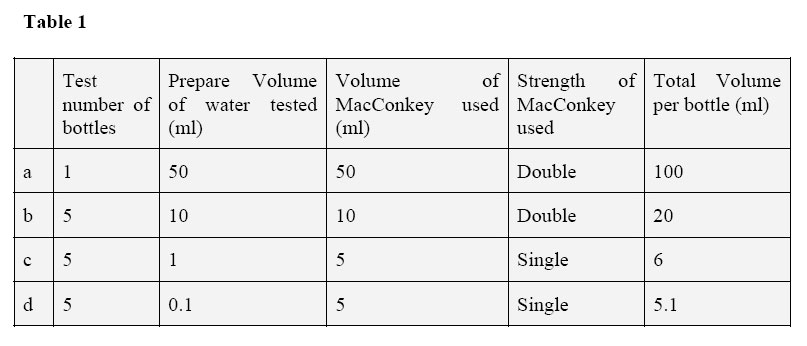
The demand for good quality water for drinking and other purposes is no doubt exceeding supply especially in some regions of developing countries where drought has claimed thousand of lives and inflicted economic and social damage1. According to World Health Organization (WHO), two thirds of diseases affecting people worldwide are of water-origin. Polluted water may contain pathogenic bacteria, protozoan, viruses or eggs of helminthes, which are known to cause serious health hazards in humans 2,3. However, for water to be potable it must be microbiologically safe and in order to achieve this, an approach that will eliminate pathogenic organisms from source water supply must be ensured. In most developing countries particularly Nigeria, the various state governments are responsible for monitoring and determining the quality of water supplied. This policy has raised a lot of questions on the efficiency and quality of water supplied to the public. Water treatment plants are the most essential and direct means of controlling the microbial quality of drinking water. However, many water treatment plants designed for and constructed in many third world countries have inherent operational problems such as sedimentation tanks which cannot be drained, sand filters are prone to flooding, non-functional chlorinators, and inadequate provision of laboratory facilities4 .The implication of these problems is that treated water drawn from taps even within the premises of most treatment plants is not entirely devoid of organisms. In the last two decades, there has been an increase in the number of reported cases of water-borne diseases such as typhoid fever, cholera and dysentery. These cases are reported .in both print and electronic media without any known fact on the predisposing factors that might be responsible for such disease upsurge in Lagos, Nigeria. Availability of safe potable water is considered to be a luxury and far from reach by over 80% of the total population belonging to the low socio-economic class where many still depend on untreated waters for their survival. The Lagos State Water Corporation (LSWC) is the sole agency responsible for public water supply to about 15 million inhabitants of Lagos State. The Corporation has several water works scattered all over the five divisions in the state. The water works are classified into surface and underground water sources. The three major water works are Adiyan, Iju and Ishasi, which make use of surface water as the water source and are responsible for about 95% of the total daily production. The remaining 5% supplied to the public are by mini-water works, which make use of underground water source (boreholes). Adiyan and Iju water works use virtually the same treatment principles but the only difference is that while sedimentation in Adiyan is vertical, Iju water works used both vertical and horizontal sedimentation (settling process). The sequences of treatment in both water works include screening, coagulation, flocculation (aluminum sulphate and polyelectrolytes) sedimentation/settling, aeration, sand filtration stability at the saturation pH and disinfections 5. The Ishasi (third main water works) and the mini-water works used the following treatment principles: coagulation and flocculation, sedimentation (vertical), filtration (sand and carbon) disinfections pH correction and storage/discharge to distribution network6. For each of the three main water works, the average plant abstraction capacity of between 4.3 to 4.5 million gallons per day and production capacity of about 4.0 million gallons per day could no longer meet the demand of Lagosians for pipeborne water supply. This situation has lead to a rise in the number of people using well waters, which are scattered all over Lagos. There has been an increase lately in cases of food and water borne diseases in Lagos, particularly typhoid fever7. Apparently lack of information on the bacterial content of source of drinking water in Lagos has made it difficult to link this febrile disease with the quality of drinking water in Lagos State. In line with this, the present study was undertaken to investigate the incidence of enteric bacterial pathogens in tap and well waters that serve as major sources of drinking water in Lagos, Nigeria. To the best of our knowledge this is one of the few reports if any on the bacterial content of well and tap waters in the last two decades in Lagos, Nigeria. Methods A. Study area and sampling: Drinking water from eighteen towns in Lagos State was randomly collected for bacteriological analysis for a period of 18 months. These areas are Oyingbo, Oshodi, Mushin, Ojo, Iwaya, Amukoko, Ijesha, Makoko, Ajegunle, Ipaja, Bariga, Oworonsoki, Ketu, Ikeja, Agege, Surulere, Ijanikin and Yaba. These towns are mainly inhabited by low and middle socioeconomic classes, which constitute about 80% of the total population of Lagos State. Tap and well waters constitute the source of drinking water in these areas. Indiscriminate dumping of household wastes along the water supply pipelines was noticed in some of these areas, pipeline leakages were also paramount. All the wells under study were owned by private individuals and are usually open to general public. While some of the studied wells were covered, many were not. Drawing of water from these wells was by the use of 5 – 7 litres containers, which is either tied directly to the well cover. In some cases, where this is not possible, individual fetchers usually come with small bucket to draw water. The wells are 20 years old, some were constructed with concrete cements, and are on average five meters deep. B. Collection of well water samples: Water samples were collected in sterile bottle tied with a strong string to a piece of metal (about 500g) as the weight. The bottle cap was aseptically removed and the weighted bottle lowered into the well to a depth of about 1-2 meters. The bottle was brought up to the surface and covered with a screw cap when no air bubbles were seen inside. All bottles were immediately labeled and were brought to the laboratory in cold box for bacteriological analysis. C. Collection of tap water samples: The tap water used in this study was chlorinated from the water works. Neutralization of chlorine was done using standard methods8. In brief, 0.1 ml of 1.8% (W/V) solutions of sodium thiosulphate (Na2 S2 O3 .5H2 O) per 100ml of bottle capacity was used. In some cases where lower volume of water was used, appropriate level of sodium thiosulphate solution was added to the bacteriological sample bottles before they were sterilized. All external fittings such as anti-splash nozzle or rubber tube were removed and the tap nozzle cleaned properly. The tap was opened and the water was allowed to run-to-waste for about 2-3 minutes so as to allow any stagnant impurities in the pipe to flush off, after which the tap was later turned off. A piece of cotton wool soaked in methylated spirit was held with a forceps which was ignited with a piece of match was used to heat-up the tap nozzle until it became unbearably hot to touch to ascertained non contamination from external source. The tap was then allowed to run continuously for about 1 minute so as to cool the water after which a pre-labelled sample bottle was filled from the gentle flow of water from the tap and the screw cap carefully replaced. All samples bottles were also brought to the laboratory in cold box for bacteriological analysis. D. Bacteriology: The multiple tube fermentation technique as described by Mackie & McCartney9 was adopted. In brief, varying quantities of the water samples were added to McCartney bottles containing MacConkey broth (Oxoid) of different strength, with inverted Durham tube in each bottle. The details were as shown in the Table 1. For presumptive test a combination of a, b and c was used for well waters and that of b, c and d was used for tap water. The tubes were incubated aerobically at 370C for 18-24 hours. Sterile distilled water was used as a control for each test batch. Presumptive Coliforms count was obtained by making a reference to the MacCrady’s probability table. The most probable number (MPN) of Coliforms per 100ml of water sample was computed from various combinations of positive and negative results obtained from the test tubes. E. Identification of Isolates: Subcultures were made from positive tubes of the presumptive test on to Eosin methylene blue agar and MacConkay agar (Oxoid) for the enumeration of Escherichia coli and Enterbacter aerogenes. Salmonella spp and Shigella spp were enumerated using Salmonella – Shigella agar followed by sub culturing of non- lactose fermenting colonies on triple sugar iron agar (Oxoid). All the inoculated media were incubated aerobically at 370C for 24 hours. Isolates were then identified by combination of colonial and morphological characterization on solid media together with standard biochemical reactions as described by Cowan and Steel10. Results
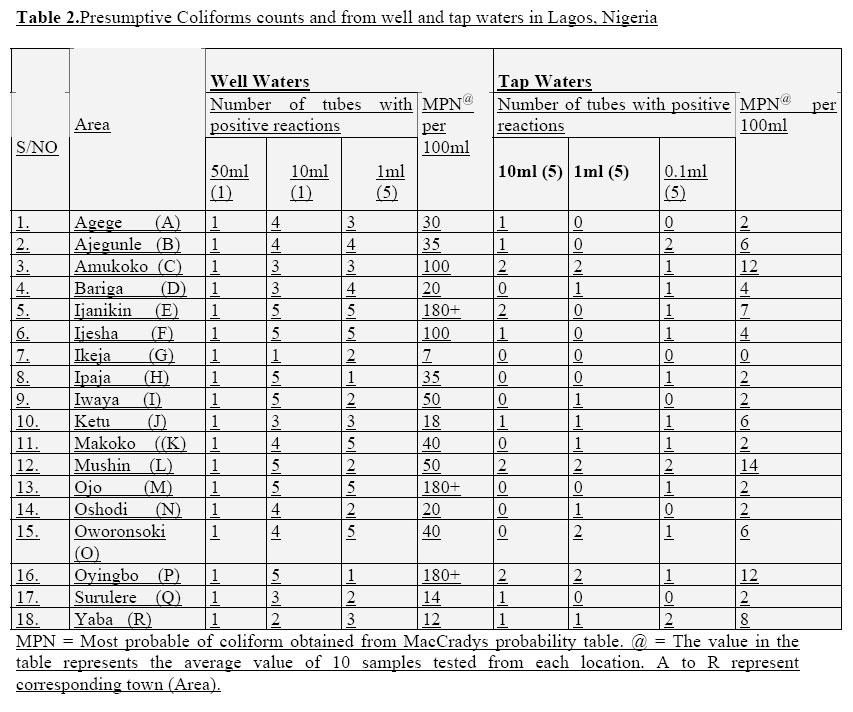
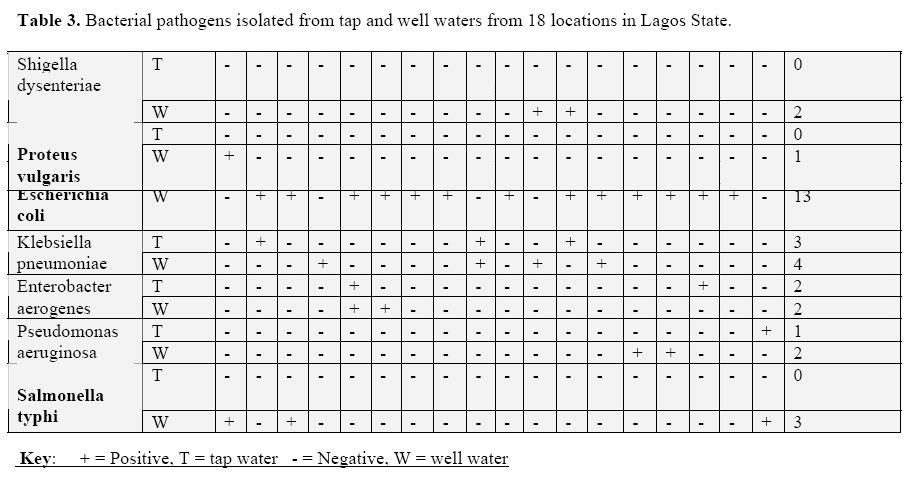
The result of the presumptive Coliforms test for the multiple tube technique of bacterial enumeration of well and tap waters are clearly indicated in Table 2. The MPN per 100ml for well water samples ranged between 7 and 180 colonies, which exceeded the standard limit set by The World Health Organization (WHO). Eight samples of the 18 tap water locations were found to contain bacterial counts ranging from 6 to 14 colonies per 100ml of tap water sample ranging (Table 2), which also exceeded the standard limit set by WHO. Table 3 showed bacterial pathogens isolated from both tap and well waters from different locations. Nine well water samples from the tested locations contained two or more species of bacterial pathogens. Escherichia coli was the most frequently encountered in 4 tap water samples and 13 well water samples followed by Klebsiella pnenumoniae encountered in 3 tap water samples and 4 well water samples. Other pathogens isolated from well water samples are Enterobacter aerogens (2), Pseudomonas aeruginosa (2), Salmonella typhi (3), Shigella dysenteries (2) and Proteus vulgaris was the least encountered (one well water sample) (Table 2). Surprisingly, one or more of these bacterial pathogens were isolated from tap water samples from the following sample locations: B, C, E, I, L, O, P and R (Table 3). However, no S. typhi, S. dysenteriae or P. vulgaris was isolated from any of the tap water samples in this study. Discussion The transmission of disease through consumption of facally contaminated waters particularly in developing and under-developing countries has long been recognized and documented 3,11&12. In Lagos, Nigeria, provision of safe potable water to the public by government is rare and restricted to few estates mainly inhabited by the high socioeconomic class of the population. Even at these estates, the public water supply is quite irregular and many individuals dig boreholes to store water. The low socioeconomic class, which forms the majority of the city population, can’t afford the additional cost of boreholes digging. As a result of the indispensability of water to human existence, most households are left with no other alternative than to dig wells as their source of drinking water and for other uses. Our findings revealed that all the well waters from the locations under study were contaminated with one or more bacterial pathogens. In contrast one or more pathogens were isolated from tap water in 8/18 sample locations (Table 3). These results clearly indicated nonconformity of both samples (Well and Tap waters) with the WHO standards recommendation for safe potable water 12; a guideline that is being adopted by National Agency for Food and drug Administration Control (N A F DAC) in Nigeria. Therefore, a situation where enteric pathogens are grossly isolated from waters consumed by human is a serious problem and should alert the authority of a possible future water-borne diseases outbreak that most probably will affect the health. Escherichia coli was the most frequently encountered pathogen in this study with more isolation in well than tap waters (Table 3). The isolation of pathogens from the tap water from some locations may be attributed to leakage of old unrepaired pipes, based on our observation of gross vandalization of water pipes in sample location B, C, I, L, O P and R (Table 2) where contamination of chlorinated tap water occurred. In other parts of Nigeria for example, K. peunmoniae and P aeruginosa have been isolated from public water supplies4 and had been attributed to possible burst along water pipe lines or unhygienic handling of water from the treatment plants. A similar situation seems to have arisen in Lagos because these pathogens were isolated from tap water samples where pipelines leakages were observed. In Lagos state and probably other states in Nigeria, the recommended chlorine-based disinfectant is the major water treatment to prevent microbial re-growth and therefore should provide continual protection to the distributed water from the treatment plants to the tap13. However, in this study, we noticed that contamination of public water supplies from the few functional government water-plant is still a common experience. The contamination may be attributed to public vandalization of water pipes, leakage of old unrepaired pipes and even particles from the water corporation. In other countries, isolation of E. coli, Enterobacter alkaligenes, E. cloacae and other pathogens from chlorinated tap water has been documented14 while E cloacae was not isolated in this study. Interestingly, S. typhi, S. dysenteriae and P. vulgaris were only isolated from well waters and none from tap water in this study. The gross contamination of well waters with these pathogens in some of the locations particularly C, E, L, O and P might probably be attributed to one or more of the following identified reasons.
The high morbidity recorded from diseases such as diarrhea, dysentery, and typhoid fever7, 15 reported lately in Lagos may be due to the consumption of such contaminated well waters. The implication of this is the increasing widespread of water and food borne diseases in Nigeria and possibly to the neighboring countries if the water sources remain unchecked. Conclusion
Constant monitoring of drinking water in Lagos to meet with WHO standards and improvement in household hygiene are essential to prevent and control cases of waterborne diseases. Moreover, government should prioritize its policy on provision of safe potable water to the public in many parts of Lagos to support the growing population There is urgent need for maintenance and replacement of worn-out facilities at water corporations to eliminate the improper water treatment from treatment tanks, prompt repair of leaking pipes and the continuous checking of proper sewage disposal into the waterways. Government should not also compromise the need for proper disposal of both domestic and industrial waste/effluents in order to prevent the epidemics of debilitating waterborne diseases in our community. In the past decades, several efforts were made especially by some international organization such as WHO, World Bank and the Pan American Health Organization (P.A.H.O) to address the problem of community health and environmental sanitation as a means of reducing water-borne diseases in developing countries. We therefore strongly recommend the efforts by these organizations to support fellowship to Nigeria in the area of potable water supply. This will not only help the control of risk of water-borne diseases in Nigeria but it will also prevent the spread of water-borne diseases to other countries by emigration and work in this region. This is the first report on well and tap waters situation in the last two decades in Lagos, Nigeria. Acknowledgement We hereby acknowledged the financial support for this study by; The Ford Foundation through the Center for Development and Democratic Studies of Lagos State University (LASU/CDDS). References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06025t1.jpg] [js06025t3.jpg] [js06025t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}