 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
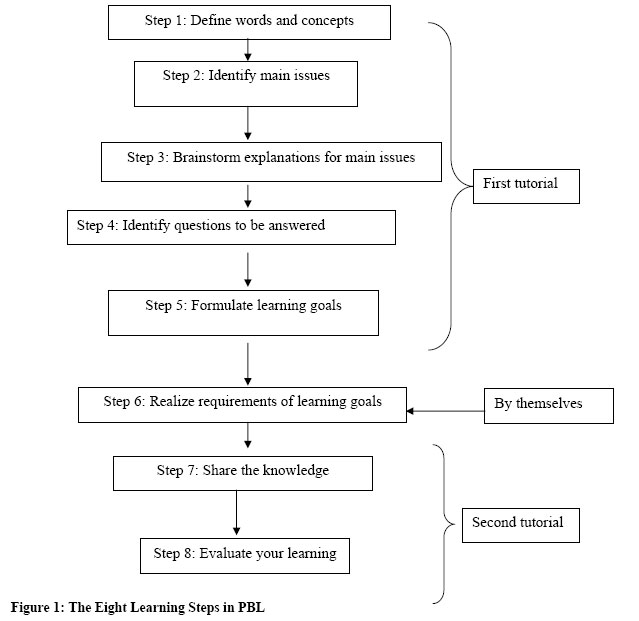
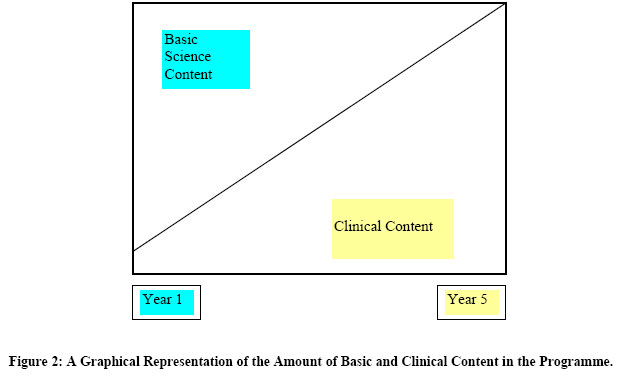
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 3-9 Problem Based Learning at the Nelson R Mandela School of Medicine J van Wyk1 BSc (Ed), B.Ed, M.Ed, T E Madiba2 MBChB, MMed (Chir), FCS (SA) 1School of Undergraduate Medical Education, 2School of Surgical Disciplines Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa. Correspondence to: Prof. T E Madiba, Department of Surgery, University of KwaZulu-Natal. Private Bag 7 CONGELLA 4013 SOUTH AFRICA. Fax: 27 31 260 4389. E-mail: madiba@ukzn.ac.za Code Number: js06027 A problem-based learning curriculum was phased in to replace our traditional lecture-based curriculum in 2001. True integration, both vertically and horizontally of the basic sciences and clinical disciplines, is reflected in each unit of learning in the first three years. The teaching programme is centrally coordinated and students work in small groups while guided by clinical and non-clinical facilitators. In the last two years, teaching and learning becomes more clinical as students rotate through the clinical disciplines. Both formative and summative assessment (including OSCE and OSPE) is used. Students have to pass each independent, clinical assessment in their final year. This paper highlights the problems and solutions of our transition to PBL. We advocate that staff and students should collaborate in the review to allow resource poor countries to find a model suitable for their unique conditions. Our programme combines the advantages of both the PBL and the traditional pedagogies. Introduction Problem-based learning (PBL) represents a major development in higher education practice1 . In PBL the curricular content is organised around problem scenarios rather than subjects or disciplines. While the early PBL literature reflects the original development in medical education at universities such as McMaster (Canada), Maastricht (Netherlands), Linköping (Sweden), and Newcastle (Australia), this instructional methodology has also become widely used in higher education 2 . The primary philosophy of PBL is the development of self-direction in learners, which promotes a culture of active, lifelong learning. The Integrated Curriculum at the Nelson R. Mandela School of Medicine In January 2001, the Nelson R Mandela School of Medicine (NRMSM) of the University of KwaZulu-Natal, Durban, South Africa, implemented a 5-year integrated PBL curriculum. It commenced after a four-year period of preparatory discussions, faculty consultations and decisions on issues of content and structure. It replaced a traditional 6-year, lecture-based curriculum in which the first three pre-clinical years preceded the last three clinical years. The traditional, didactic curriculum was characterised by an abundance of lectures, as students often needed to be reminded of content covered in prior years. The new integrated, PBL curriculum is characterised by being student-centred, selfdirected and patient-oriented with horizontal and vertical integration reflected in the merged clinical and pre-clinical content. The different disciplines that form the basis of the medical curriculum are integrated within themes in 18 modules covering 5 years of study. Orientation Students are introduced to student life at university and the PBL philosophy in their first year during a three-week Orientation programme. They are also presented with an overview of the students support structures such as financial aid, the clinic and counselling facilities. The Orientation is concluded by a short theme that relates to HIV and AIDS. Additional courses in computer literacy, English and Zulu and the Basic Emergency Care (Ambulance) Course are offered to all first year students. Students are taught and assessed in the skills of the Ambulance course. They conclude this course with a weekend-long practical attachment with the ambulance service, an assignment in the Trauma theme and a licensing exam at the end of their first year. Themes The themes or learning units are mostly 6 weeks long, while some vary between 4 and 8 weeks. Each theme typically has a common strand or focus e.g. cardiovascular disorders and both the relevant basic science concepts and clinical application are discussed in the theme. The student cohort is divided and allocated (in groups of 10) to a trained facilitator for the duration of a theme. Two tutorials are scheduled per week to discuss one/two case scenarios. A small group tutorial session is typically planned for a two-hour session with the functions of chairperson and scribe being rotated amongst the group members. The students’ learning starts with a case scenario to trigger their curiosity and to help focus their attention on pertinent learning issues that had been identified by an interdisciplinary theme design team. The clinical case scenarios require students to brainstorm the pathology, clinical approach and management. The group follows steps 1 to 5 of the 8-step protocol (Figure 1) until they have analysed the case and have identified the learning issues needed for their research. The students use the period of about five days, between the two facilitation meetings, to research their learning goals and attend interactive large group resource sessions (LGRS) where discipline experts explain concepts and principles relating to the case. Although the LGRS resembles didactic lecture-based sessions, they differ in that it requires greater student-staff interaction and it promotes the teaching of concepts and principles needed by students to understand their case. These sessions are therefore not scheduled as frequently as traditional lectures. Students also attend practical and skills sessions relating to the theme. Skills are initially taught in the faculty-based skills laboratory before being revised in the hospital wards. At the end of this period students gather for the second tutorial session where the group concludes steps 7 and 8, which require that they share their findings in order to demonstrate understanding of the case. During step 8, the functioning of the group, facilitator, chairperson and scribe is evaluated and verbally discussed. Theme design The theme is designed by a theme design group, consisting of various faculty and discipline members under the leadership of a theme head. The group identifies the core learning objectives of the theme and the principles and concepts for discussion at the LGRS. They also construct the case scenarios with its associated learning objectives and decide on relevant clinical and practical skills to be included in the theme. The design team often identifies health related sites in the community, from which students would benefit during a day-visit or an observation period such as a Hospice, hospital wards or clinics. Facilitators Facilitators are clinical or non-clinically qualified academic staff members with the responsibility to facilitate the learning process of the small group. Facilitators undergo extensive training during which they are introduced to the educational principles of PBL, the learning expected of students in this pedagogy, as well as aspects dealing with group dynamics and educational management. They are not expected to share their expert knowledge or present mini-lectures to their individual groups, but they encourage critical thinking, monitor adherence to the 8-step approach, and promote self-direction in individuals and co-operation within their group. Coordination of the PBL curriculum A faculty-based School of Undergraduate Medical Education (SUME), consisting of academic and administrative staff, was established to oversee the coordination, implementation, evaluation and review of the integrated programme and its components. Staff from the SUME coordinates the allocation of students to groups, help to recruit members for design teams, serve as year coordinators, coordinate assessment in the first three years and train and evaluate facilitators. Medical educators in the SUME also offer staff training, coordinate the academic development and mentoring programmes for students and perform evaluative functions on the quality of teaching and learning in the faculty. Problems encountered During the planning phase it was envisaged that staff would become available to teach in the PBL curriculum as the traditional curriculum was being phased out. The implementation of the PBL curriculum, however, required a much larger number of academic staff to facilitate, which coincided with changes in our health care system that impacted on travelling time, as more peripheral teaching sites had to be used. Furthermore, teaching in clinical years is based on the apprenticeship model where students accompany clinicians in hospital wards. It became impossible for clinical staff and students to adhere to a PBL timetable since clinicians were also expected to continue with their clinical work while they offered bedside teaching. This resulted in only a few clinicians becoming available to act as facilitators. Bedside teaching also does not allow for the patient to wait in the ward for a week while students brainstorm and research the subject in preparation for the second tutorial. Furthermore, non-clinician facilitators were not trained in giving clinical guidance to students in their groups, which caused concern to both clinicians, and students. The practice of small group teaching required a large number of tutorial rooms, which the physical structure of our building did not provide initially. The faculty addressed this need by renting temporary prefabricated rooms while more permanent tutorial rooms were constructed from previously used laboratory spaces. Alterations were also made to the library to accommodate students’ new way of learning. Approximately 50% of our students come from high schools where teaching was teacher centred while most of our staff also trained in the didactic mode. Staff and students are thus relatively unfamiliar with self-directed learning and the PBL methodology. Some students likened self-directed learning to “learning by correspondence” especially where the degree of guidance provided by the experts became questionable. This led students to the perception that the PBL degree would be inferior to that of the traditional curriculum. Both students and academics highlighted the lack of basic science knowledge of students in the first three years. This could be due to the limited number of basic science lectures and practicals in subjects such as anatomy and physiology during the first two years. Themes and bedside teaching, offered in the clinical years, thus highlighted the student’s lack of adequate understanding of basic science concepts when the patient as a whole was discussed. Addressing the problem The faculty embarked on curriculum workshops in which academics and students participated in frank discussions to find suitable solutions for the identified problems. These resulted in modifications to the curriculum and in some cases additional sessions were scheduled to address these shortcomings. Students from both the PBL and traditional programmes needed a lot of assurance that the MBChB degree emanating from these curricula resulted in the same outcome, despite the apparent difference in teaching approaches. This concern was eventually alleviated for those in the 5-year, PBL programme when full accreditation by the Health Professions Council of South Africa obtained in 2005. The current curriculum is, however, still being modified. The first three integrated years are theme based and the last two are more discipline-based. A 9-week foundation theme had been introduced to provide a firmer basic science foundation. The clinical sciences gradually increase in prominence and the emphasis on basic sciences decreases until, in the later years clinical application predominates (Figure 2). The objective is not to forget the basic sciences but for the students to use prior basic science knowledge and apply it to clinical concepts. This spiral nature of the programme ensures that concepts are revisited and expanded upon from the first to the final year. Students rotate in their fourth and final years through various clinical hospital-based departments where they apply and consolidate concepts that were introduced earlier. The clinical departments through which they rotate are Medicine, Surgery, Psychiatry, Obstetrics and Gynaecology, Paediatrics, and Family Medicine. Training in the surgical disciplines during the first three years of PBL forms part of the integrated curriculum and the academic staff from these disciplines participate in the different activities of each theme. Students rotate through the surgical specialities for a period of two weeks in their fourth year. In the final year of study they rotate through the Department of General Surgery (including Orthopaedic Surgery) for a 6-week period. The teaching is at the level of the generalist in the final year. No lectures are presented to final years but students participate in tutorials and bedside teaching where they consolidate their prior knowledge. Assessment Both formative and summative assessments are used in the first three years. The assessment activities of the first four years are administered by academics in the SUME. The methods used are Objective Structured Clinical Examination (OSCE), Objective Structured Practical Examination (OSPE) and case-based written examinations. In the last two years students are assessed on core knowledge and skills at the end of each clinical 6-week block. Discussion The objectives of the curriculum include an attempt to encourage students to become self-directed learners, critical thinkers and problem-solvers with the ability to ask appropriate questions, search for relevant information and ultimately to use this information efficiently. Furthermore learning around clinical cases simulates authentic contexts for medical students while they develop clinical thinking skills. It is envisaged that deep learning and independent investigation of learning issues, which characterises PBL, encourages self-directed approaches and an easier adaptation of medical practitioners to the changing health care needs of society3-6. Students should thus come to understand the process of clinical reasoning which should take precedence over memorisation, rote-learning and factual recall7. The conversion to PBL at our school was supported by educational studies which found that students are better able to integrate new concepts after identifying their prior knowledge and that learning becomes more meaningful when students understand the relevance of their learning4,7. There is evidence that students in PBL curricula use a greater number and variety of resources than their counterparts in traditional curricula8-10 . Graduates from PBL schools additionally report a greater preparedness for medical practice in domains such as independent learning11-13 . Vernon and Blake14 compared the scores of PBL students and those of students trained in the traditional programme on tests of factual and clinical knowledge in medical education and found no significant differences. They, however, noted significant superiority of PBL students with respect to their clinical performance and attitudes towards their curricula. A recent meta-analysis1 showed that PBL students experienced less distress, anxiety and hostility as the teamwork approach encouraged collaboration rather than competition amongst group members. PBL students also displayed positive outcomes when assessed for understanding of principles that linked concepts and they reported more satisfaction with their learning experiences. Interestingly a review of 183 studies15 showed that effects of prior knowledge in PBL on students' performance varied as a function of the method of assessment. We believe that the reluctance of clinical staff to adopt the PBL methodology in our faculty was multifactorial. Teaching clinical aspects to students who lacked understanding of basic science concepts early in their educational career was an obstacle because it frustrated educators and de-motivated some students. The difficulty experienced by clinicians to conform to the PBL timetable, which required predetermined facilitation meetings, might also explain the lack of clinician buy-in. Furthermore, the integration of disciplines and central coordination of student activities resulted in a degree of alienation of departmental staff that now no longer cared for students for prolonged periods. This caused many staff members to feel less accountable and less responsible for the students and their learning. Studies have shown that the shift from the ‘expert role’ of teacher to that of a facilitator ,where facilitators do not share their expert knowledge, are very uncomfortable to some lecturers16,17. Furthermore, Miflin and colleagues18 reported inconsistencies in the interpretation and implementation of self-directed learning by staff in some faculties, resulting in some interpretations being counterproductive and instead causing students to become overly dependent on academic faculty staff for direction and guidance. Evidence, on the other hand, suggests that PBL is favoured by faculty who are trained in the facilitatory approach19. Despite the fact that many lecturers doubt the abilities of their students to adapt to self-directed approach as required in PBL, most students have succeeded in making the transition, especially with the appropriate support by committed tutors20. Things that thus needed urgent attention were the inflexibility and cost in terms of time, staff and building alterations. Despite Sefton et al’s21 findings that offerings in PBL would not be more costly to faculties than traditional teaching, we experienced the contrary, especially because our class sizes exceeded 200 students. We also agree with authors who suggest that a PBL curriculum requires considerable planning, foresight and communication and that sustaining such reform present more difficulties than the initial implementation 22,23. Another important consideration for faculties implementing PBL is the establishment of a well structured staff development programme to support the educational changes expected from its staff24, particularly as even experienced facilitators still need continuous support and training 16,22,25,26. In a faculty such as ours with limited resources of educationally trained staff, it is important to have a dedicated medical educational team and skilful timetabling. An additional requirement would be to convince staff developers to also oversee other duties (i.e. evaluations, assessments, coordination) apart from the student and staff supporting functions. Widely varied methods have been used to assess students’ learning in PBL ranging from traditional multiple-choice and essay examinations to new assessment techniques such as case-based assessment, self-and peer assessment, performance based assessment and portfolios. It is paramount that a valid assessment system evaluates students' problem-solving competencies in an assessment environment that is congruent with the PBL environment. It should also consider both the organization of the knowledge base and the students' problem solving skills27 which justifies our continued use of the OSCE, OSPE, and written, oral and clinical examinations. Evaluation of the overall curriculum and its contributing parts should therefore be a priority for curriculum designers in order to determine the factors that contribute to the sustainability of the reform. Failure to do so will ruin the reputation of the programme and the school and its graduates can be seriously jeopardised. We were fortunate that we received the input in good time and we were able to amend our curriculum before it failed. The cooperation between staff and students and the realization by authorities that buy-in from both students and staff was critical in bringing a turnaround in our curriculum. The PBL curriculum at NRMSM will need to be re-evaluated after a few years of practice to ascertain whether the learning objectives of the programme have been achieved in practice. Conclusion The purpose of our integrated curriculum is to produce a generalist. The discipline of surgery, like other disciplines, participates in the planning and implementation of the themes where new information is initially presented and later revisited to cement the students’ knowledge base. In the last two clinical years, students rotate through General Surgery to consolidate the knowledge already gained in previous years and to concretise their approaches to surgical conditions. A graduate in General Surgery should therefore understand surgical principles, be able to identify surgical conditions and know when to refer patients for specialised care. The PBL curriculum has been demonstrated to produce graduates with positive attitudes towards PBL itself. Acceptance of the curriculum by students and faculty staff is varied. The integrated curriculum at the NRMSM seems to accomplish the objectives of PBL as well as the proven accomplishments of the apprentice system of the traditional methods of teaching. As with all innovations, our PBL curriculum has had teething problems, which necessitated some modifications. We are, however, committed to regular review. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06027f1.jpg] [js06027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}