 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
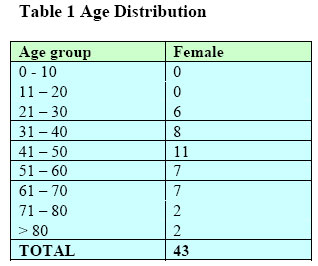
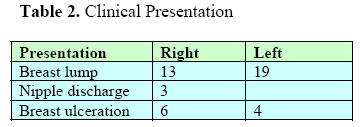
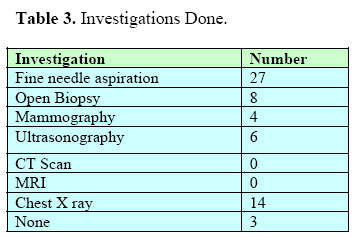
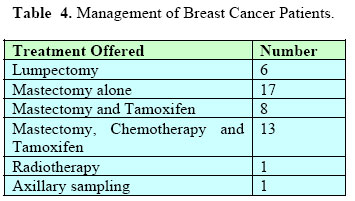
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 10-14 Breast Carcinoma at Coast Province General Hospital- Mombasa Kenya G.G.O. Calleb MBChB MMed FCS-ECSA Consultant Surgeon Coast Province General Hospital P O Box 91176 Mombasa-Kenya. Code Number: js06028 Background: The aim of this study was to determine the pattern of breast cancer in patients presenting with the disease at Coast General Hospital in Mombasa-Kenya. Introduction Breast cancer is the commonest cancer affecting women of ages 35 to 54. Less than 1% of all breast cancers affect men but this occurs at a later stage (usually in men aged 50 – 60 years)1,18. The 5 year survival rate has improved from 53% in the 1940s to over 80% currently. This has been attributed to adjuvant therapy and early detection. However the death rate has not changed. Predisposing factors include positive family history, early menarche and late menopause, spinsters, late age at first pregnancy, existing ovarian or endometrial cancer and unilateral breast cancer. Other predisposing factors that have been investigated include estrogen therapy, antihypertensive drugs, obesity, and high fat diet. Obesity and fibrocystic disease of the breasts have also been incriminated. Women who had early pregnancy below 20 years, multiple pregnancies or are of Asiatic origin tend to have a lower risk of developing breast cancer. Management of breast cancer involves surgery and adjuvant therapy. The challenge in our set up is the late presentation and inaccessibility and /or unaffordability of adjuvant therapy especially radiotherapy, chemotherapy and antihormonal agents2-7. In regions where screening programs for aggressive breast cancer are in place, the mortality has reduced by 20% since the 90s partly due to more emphasis on regular mammograms and improved treatment options3,9,17. The pattern of breast cancer at the Coast Province has not been documented but more cases of breast cancer in the under 30 years are being see. Lately, there has been an increased awareness of breast cancer after several awareness campaigns by a Kenya Breast Health Program NGO in conjunction with various Hospitals and this has resulted into many new cases presenting at a slightly early stage. This study was aimed at determining the pattern of breast cancer in patients referred to CPGH and the treatment options available to them. Patients and Methods A retrospective and prospective study of patients confirmed to be with breast cancer from January 2002 to June 2005 was conducted. Information was retrieved from the patients’ clinical notes and operative records. The information obtained included the demographic pattern, clinical presentation mode of management and follow up findings. Most patients presenting with breast lumps had FNAC done. Those confirmed to have breast cancer on FNAC and had clinically operable tumours routinely underwent mastectomy with or without axillary sampling. All the patients initially were seen at the filter clinics or at peripheral facilities and were later referred to the surgical consultation Clinics. All cases were managed under the supervision of a consultant Surgeon. A patient who has diagnostic FNAC is started on adjuvant hormonal therapy immediately after presentation. Chemotherapy when available was commenced 2 weeks after surgery. Follow up was done routinely every three months.Most patients presenting with breast lumps have FNAC done and if breast cancer is confirmed they routinely undergo mastectomy with or without axillary sampling. Patients who present with advanced carcinoma (ulcerating) undergo toilet mastectomy without FNAC with delayed skin grafting and chemotherapy after histological diagnosis. Results All patients were females. A third (33%) was below 40 years. Twenty six (60.5%) of the patients were in the 30 to 60 year age group (Table 1). Table 2 shows the presenting features of the disease. A significant number (23%) of cases presented with late disease and had breast ulceration. there were only3 cases of nipple discharge and the right breast was mainly affected. Twenty seven of the patients had FNAC done on them (Table 3). Only 4 patients had mammography performed. Pre-operative Chest X Rays were done on less than 25% of the patients undergoing mastectomy. Ultrasound had only 6 and none had CT scan done on them. MRI is not available in Mombasa and expectedly none had an MRI performed. All patients underwent mastectomy (Table 4). Six patients who initially were done lumpectomy were on histology confirmed breast cancer and had to have mastectomy subsequently. Only 13 patients had adjuvant chemotherapy and anti-hormonal management after operation. This due to the high cost of chemotherapeutic agents and as such the patients could not afford. A good number 17 did not receive any adjuvant treatment. Ten patients had toilet mastectomy and the others had disseminated cancer. 8 had mastectomy and Tamoxifen. Tamoxifen was prescribed for all patients but most patients could not afford and depended on hospital stock whenever available. Axillary sampling was done in one of the cases. Only one patient had adjuvant radiotherapy. Using a normogram the doses were calculated as follows:-The patients who received chemotherapy were given four or six cycles of:
OR
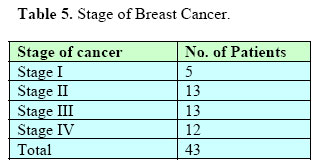
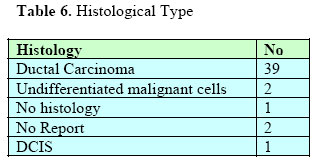
Repeat cycle every 28 days x 3 then every 3 months for a further 3 courses. Plasil and zofran were used to prevent emesis. Table 5 shows that the majority of patients presented with stage II cancer and beyond. Only 5 patients presented with stage I carcinoma. In 39 patients the tumour type was ductal carcinoma, 2 had no histological report and only one had ductal carcinoma in situ (Table 6). Two cases had undifferentiated malignant cell on FNAC and one had no histology reported, The patients on average attend clinic for 1 year after which they were lost to follow up. It was therefore not possible to determine the recurrence rate. Discussion It is apparent that only a few patients presented with early disease. The majority presented with late and as such the management is challenging with the scanty resources. This is due to lack of awareness and screening program which hopefully identify early breast cancer when it is curable and treatable. At this stage breast conservation treatment can be practicable4,5. Early detection is three pronged and includes annual mammography for females over 40 years, monthly breast examination and frequent clinical examination done by a health care provider. Individuals with a family history of cancer require special attention. Mammograms will detect about 85% of breast cancers. Computer aided Detection (CAD) is one of the adjuvant technologies that some radiologists use to spot cancers on mammograms4,6,8. A study done in a six year survey of 236 Canadian women between ages of 25 to 65 who carried BRCA1 and BRCA2 gene mutation (having 85% risk of developing breast cancer) were screened using MRI, mammography, ultrasound and manual exams. The researches found 22 cancers. MRI found 75% of these, mammography and ultrasound detected a third and breast examination found only 10%. However it has not been proven that MRI is a better diagnostic tool as the study concentrated on women with BRCA mutation gene1,15. Research on use of Laser imaging in detection of breast cancer has been done. Preliminary findings have shown the system to detect some growths not detected by mammography. Mammography however is still the first line of defence against breast cancer6,17. The primary treatment of breast cancer has been surgery. The surgery can either be breast conserving namely lumpectomy or quadrantectomy or mastectomy with immediate or delayed reconstruction. None palpable lesions can be resected after localization by guide wire; wire guided lumpectomy (WGL), placed during mammography, or by radioguided occult lesion localization (ROLL) technique17. Breast reconstruction does not alter the behaviour of breast cancer but is mainly of psychological benefit. Reconstruction may involve the use of an implant or lattissimus dorsi, transverse rectus abdominis myocataneous flap or gluteus myocutaneous flap. While the first two have vascular pedicles, the later is a free transfer and the superior gluteal vessels are anastomosed to internal mammary vessels. Is advantage is the big muscle bulk even in thin women and the ease of closing the defect and the well hidden scar. In early cancer the technique of subcutaneous (skin saving) mastectomy can be carried out. However in breast conserving surgery meticulous follow up is mandatory with regular examination by mammography, CT scanning and ultrasonography. If these facilities are not readily available then mastectomy is advised. Historically the first adjuvant therapy for breast cancer was initiated by George Beatson and A Schinzinger1 who observed remission in premenopausal women with breast cancer by doing oophorectomy 100 years ago. In our set up all cases of breast cancer are managed primarily by mastectomy. This is followed by a 4 or 6 cycles of chemotherapy. Commonly used regimen is CMF or CAF. Tamoxifen is used for hormonal therapy for 5 years. Aromatase inhibitors are effective for postmenopausal estrogen receptor positive advanced breast cancer; indeed some studies have shown that in early node negative cancer Tamoxifen or Arimidex may be used instead of chemotherapy. A further justification in the use of Tamoxifen is that it reduces local recurrence in oestrogen positive cancers in both premenopausal and post menopausal women. Arimidex is recommended for premenopausal women as Tamoxifen does not work on the ovaries1,2,5,10. Radiotherapy is indicated after surgery to prevent recurrence. 27% of patients develop local recurrence if no adjuvant radiotherapy is given especially in node positive (high risk) cases. Where there is local recurrence radiotherapy is indicated provided there was no prior radiotherapy. Postmenopausal women with recurrence who previously did not receive Tamoxifen would benefit from Tamoxifen. Local recurrence in the conserved breast has a better outcome than that following mastectomy. There are newer systemic treatments that have been found to have fewer side effects; these include taxanes in combination with anthracycline regimen. Herceptin has been found to be effective in women whose tumour is HER-2 positive. HER2 receptors tend to occur in women who have poorly differentiated Oestrogen-receptor negative tumors who are node positive. Breast cancers respond to chemotherapy in differently. It is difficult to predict which women would derive additional benefits from chemotherapy and which ones would not. The policy therefore is that when in doubt chemotherapy should be given. Recent studies have shown that a new genetic test, Oncotype DX 21-gene assay not only assesses the likelihood of recurrence for many early breast cancer patients, but also predicts how much chemotherapy will help these women. For women who have node negative tumours, the oncotype assay analyzes 21 genes related to breast cancer including the oestrogen receptor, HER2 and proliferation genes. It then divides them into low-, medium and high-risk scores. Women on the low risk group would only require minimal chemotherapy. This test could be used to determine women with node negative hormone positive tumour who would do well with Tamoxifen alone and may not need chemotherapy and those who would benefit from chemotherapy6. Management of breast cancer is a fast changing discipline with specialized breast centers for management of breast cancer. There are also screening programs and active research going on the role of hormonal manipulation as adjuvant therapy either a lone or in combination with chemotherapy in pre- and post-menopausal women. There are on going trials examining combinations of oophorectomy (by surgery or radiation), ovarian suppression using LHRH or GHrH analogues, Tamoxifen, and chemotherapy in premenopausal women. In postmenopausal women, studies on the role of aromatase inhibitors, either alone or in combination with Tamoxifen are underway. The results of these trials may change the approach to the management of breast cancer in the next 2 to 5 years. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06028t3.jpg] [js06028t5.jpg] [js06028t4.jpg] [js06028t2.jpg] [js06028t1.jpg] [js06028t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}