 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 15-20 Radionuclide Scan and Other Diagnostic Studies in Goitre Patients in Tanzania E.T.M. Nyawawa, S. Yongolo, J. Tupa Department of Surgery, Muhimbili University College of Health Sciences and Consultant Surgeon Muhimbili National Hospital / Muhimbili National Hospital Code Number: js06029 Background: Since the introduction of radioactive isotope scanning facilities in Tanzania, there has been no study to determine in the usefulness of this modality in evaluating the pattern of goiters. The aims of this study were to determine the pattern of radionuclide scan, its accuracy in diagnosing the nature of the lesion of a thyroid disease and comparing this with other available diagnostic techniques. Introduction Thyroid scintiscan has in the past been a widely used screening procedure in evaluation of thyroid nodules since it was described more than 45 years ago. It was suggested that thyroid carcinoma concentrated less radioactive iodine than did normal thyroid tissue1 Thyroid radionuclide scan may also be contradicting in relation to uptake of radioactive isotope between the normal and pathological lesions2 . Distinguishing between benign and malignant disease of the thyroid is not usually easy and in turn poses management difficulties. The prevalence of thyroid nodules in USA is reported to be 4-7%3 . When diagnosed by ultrasound the incidence raises to 30-50% 4,5. Fine Needle Aspiration Cytology (FNAC) is accepted at present as the most precise diagnostic screening procedure for differentiating benign from malignant thyroid nodules6 . It is safe, inexpensive and accurate in experienced hands; it has a sensitivity of 90- 92% and specificity 74-83%, with few false positive 3.3%. However this high sensitivity and specificity may not represent the same picture between developed and developing population. Considering the differences in socioeconomic and peoples awareness with regards to health, it is clear that majority of patients from developing countries presents late to Hospital with disease being more advanced and hence the pattern of thyroid disease might be different. Since the introduction of Thyroid scintiscan in this country there is increased awareness by physicians to utilize it as one of the diagnostic tool in patients with goiters: However there has been no evaluation since isotopic scan was established in the country. The aim of this study was to determine the pattern of thyroid scan, the nature of the lesion and compare with other conventional diagnostic technique in patients presenting with goiter in a tertiary hospital. Patients and Methods This was a retrospective, case finding study in which all patients with goiter who underwent surgical operation between June 2000 and July 2003 are included. The files of these patients were retrieved from the hospital record department. Out of a total of 134 patients who underwent thyroidectomy 124 were enrolled for the study. Excluded were those whose did not have Radionuclide scan. Patients’ initial clinical evaluation was reviewed and age sex, duration of symptoms and clinical diagnosis were entered into a questionnaire. The type of investigation done followed this. The thyroid scan report was reviewed to note whether there was increased uptake (hot), isofunction (warm) or whether there was no radioisotope uptake (cold). The reports of FNAC were also noted and finally the type of thyroidectomy the indication for surgery and the final histopathology report of the thyroid were recorded as benign or malignant (follicular/ papillary carcinoma) Patients, data were entered into an epinfo2000 program and analysis done. However the study was limited because of lack of experienced cytopathologists and it was a retrospective. Results A total of 124 patients with goiters who underwent surgical operation between June 2000 and July 2003 were enrolled in the study. There were 106 females and 18 males patients with goiter constituting a male to female ratio of 1:6. Most patients were in the age group of 3140 and 41-50 years. The mean and median ages were 42.7 and 42.5 years indicating normal distribution. The minimum age was 13 years and the maximum was 72 years with a standard deviation of 12.27 years (Table 1). The mean duration of symptoms was 4 years, median duration 3 years with a range of 1-20 years. Table1. Patients age groups.
Malignancy was found in 23 patients making an overall incidence of malignancy of 18.6%. There were 60 (48.4%) patients whose thyroid scans demonstrated ‘cold’ lesions. Malignancy was found in 21 (35%) cases of patients with cold lesions: of which 9 (15 %) had follicular carcinoma and 12(20%) had papillary carcinoma. Two (3.6 %) patients out of 55 who had ‘warm’ lesion were found to have follicular carcinoma. No malignancy was found in patients with hot lesion as seen in table 2. FNAC was reported insufficient in 10 patients of whom 8(80%) had benign thyroid disease and two (20%) patients had follicular and papillary carcinoma one cases each. Table 2: Thyroid scan and histopathology
* Brackets indicate proportion percentage Table 3. FNAC and histopathology report
Table 4. Accuracy of FNAC in detecting malignancy and histopathology report
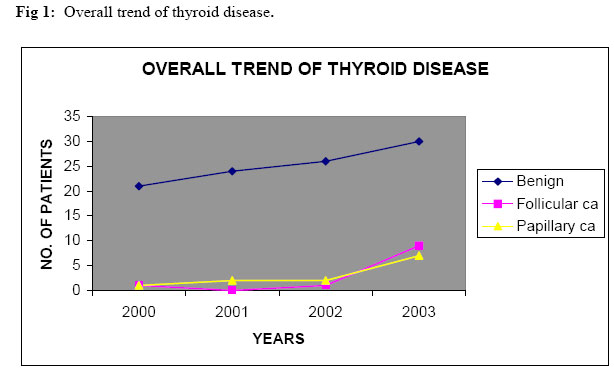
The overall sensitivity of detecting malignancy by FNAC was 66.7% and the specificity of 92.5 % (Table3). Follicular carcinoma and papillary carcinoma was found one case each in those whom FNAC had suggestive of follicular adenoma. All patients diagnosed to have papillary carcinoma by FNAC were all indeed found to have papillary carcinoma on histopathology report. Malignancy was found in 10.7% of patients who had multinodular goitre. Two (5%) patients out of 40 with colloidal goiter were found to have follicular carcinoma. The overall thyroid disease showed that benign lesions were the leading cause throughout the years while, follicular and papillary carcinoma showed a parallel trend with only a slight increase in follicular carcinoma recently as demonstrated in figure1. In almost all patients with malignant thyroid disease the indication for operation was due to suspicious lesion, except in one patient with follicular carcinoma in which it was due to pressure symptoms. Majority of patients with benign disease the indication were suspicious 41 (65.1%), All patients whose indication was cosmetic had benign disease (Table 5). Table 5: Indications Of Operation And Nature Of Thyroid Disease.
Table 6. Type of Operation and Their Indication.
NOS‡ = Not otherwise specified thyroidectomy. The majority of patients who underwent near total thyroidectomy the indication was a suspicion lesion (80%) while, the rest were due to pressure symptoms 17.5% and in one due cosmesis 2.5%. Subtotal thyroidectomy was done in nearly equal proportion in patients who had pressure, thyrotoxicosis and in those who wanted cosmesis 33.3%. Only while in one patient the indication was due to suspicion lesion 6.7% (Table 6) Discussion This study demonstrated that the risk of malignancy lesion detected in patients’ with ‘cold’ lesion on thyroid scan was higher (35%) with an overall incidence of malignancy of 18.6% (Table 2). It has been reported that approximately 80% of thyroid nodules are cold and only 10-16% of these are malignant7. In this study 48.4% of patients had cold lesions and 35% of these had malignancy. These findings is similar to other studies whereby a relatively higher incidence rate of malignancy ranging from as low as 10% to as high as 50% has been reported8,9 The clinical picture and pattern of thyroid disease seen and reported in developed countries may be different from disease pattern in third world countries especially in goiter endemic areas. This is mainly affected by socioeconomic status and literacy. The majority of patients in developed countries report to hospital early and management is given accordingly. While the majority of patients with goiter in developing countries present late as the case in this series of patients who presented at an average of 4 years the minimum time to report was 1year and the maximum was 20 years after onset of disease with symptoms of pressure, cervical adenopathy and hoarseness of the voice. Seventy four (60%) of our patients had multinodular disease and the incidence of malignancy was found to be high (15%). This may suggest that there is a higher risk of malignant degeneration in patients with long standing history of goitre10. However a higher incidence of malignancy from multinodular goiter (5-48%) has been reported in other series from developing countries in which surgery was done for cosmesis11,12. A higher incidence of malignancy in ‘cold’ lesion seen in this study suggests that a radioisotope scan though considered being secondary investigation tool in evaluating thyroid disease after FNAC might be a useful investigation option based on radioactive uptake nature for a thyroid lesion. This is because while FNAC is generally reported to have high sensitivity (74-83%) and specificity (92%) with low false positives (<5%)13,14 in our set up however this is not the case. The accuracy FNAC for thyroid disease like that reported for breast cancer (unpublished) in Tanzania has been shown to be low. In this study the sensitivity (66.7%) was low however; specificity (92.5%) was similar to other reported series. Overall benign thyroid disease is more common than malignancy: while follicular and papillary carcinoma has almost a parallel trend throughout with a slight recent increased rate (Fig 1). Reports from developed countries suggest that papillary carcinoma is the commonest malignant type (80%), follicular carcinoma (20%), medullary carcinoma (<5%) and anaplastic carcinoma (<1%)3. In this study none of the patients had either medullary or anaplastic carcinoma. Like in many other studies the usual indications for thyroidectomy in this study were cosmetic, suspicious lesion, pressure symptoms and thyrotoxicosis. All patients in whom the indication was cosmesis indeed turned to have a benign lesion while in 63 patients suspected to have malignant 41had benign, 10 follicular carcinoma and 12 had papillary carcinoma. None of the patient with thyrotoxicosis had malignant disease. One patient in whom the indication was cosmesis underwent near total thyroidectomy probably because of gross degenerative changes. The majority of patients suspected to have malignancy underwent near total thyroidectomy (80%), which is usually considered an appropriate procedure. All patients diagnosed to have thyrotoxicosis had raised T3/T4 serum levels and except in one patient the TSH serum levels were decreased. The raised TSH in that patient might be due to a hyper-functioning thyroid adenoma that is the usual finding. Conclusion This study at Muhimbili National Hospital reveals that patients report to hospital in seeking medical attention there is higher incidence of malignancy in cold thyroid lesions. There is low sensitivity for detecting malignancy by FNAC at our institution. It is suggested that radioisotope thyroid scan which is now available might be the better preliminary investigation for diagnosis of thyroid lesions before FNAC is undertaken. Acknowledgement The authors appreciate the co-operation of the staffs from medical records that were helpful in facilitating to obtain patients’ case notes and hence retrieving patient data. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06029f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||


{kind=link}