 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
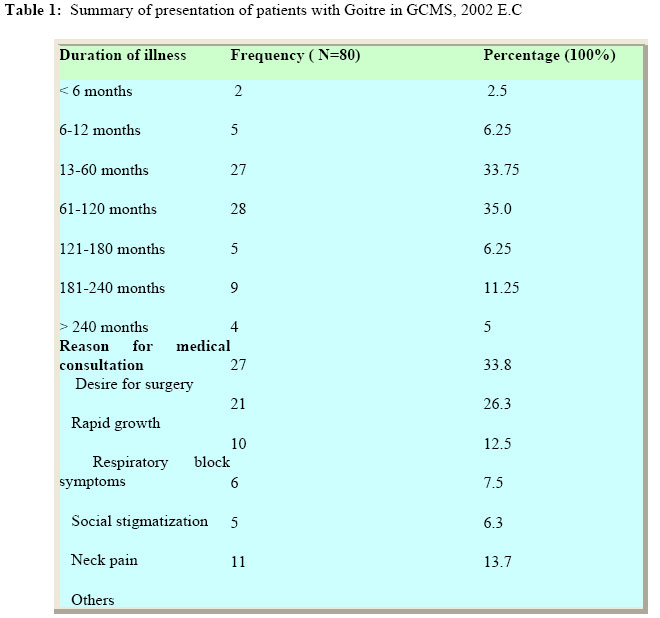
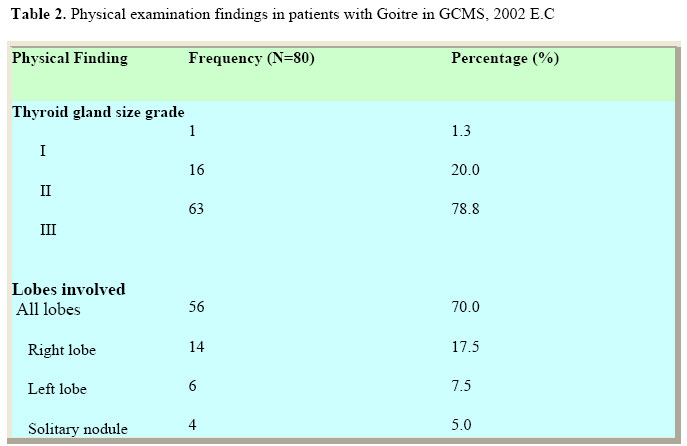
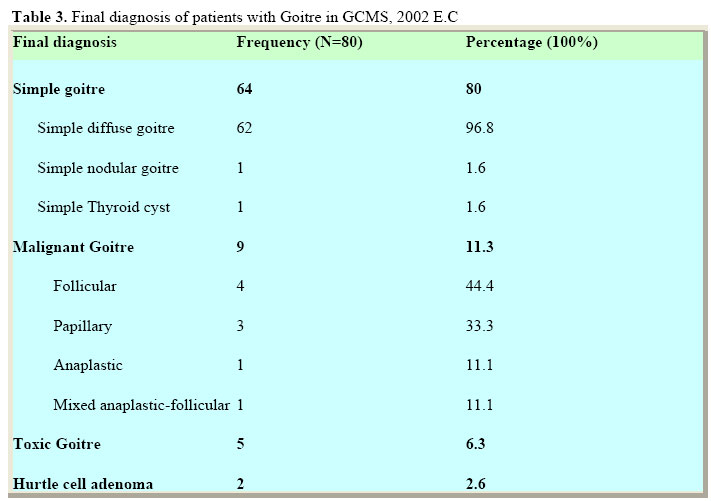
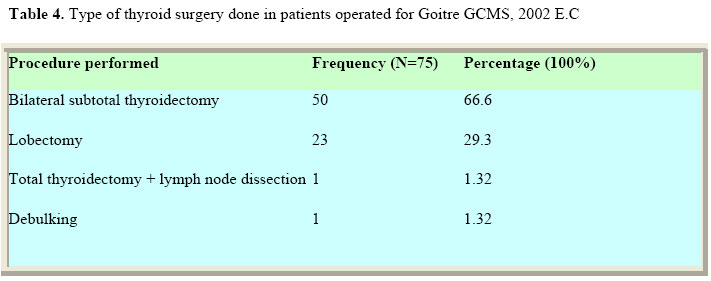
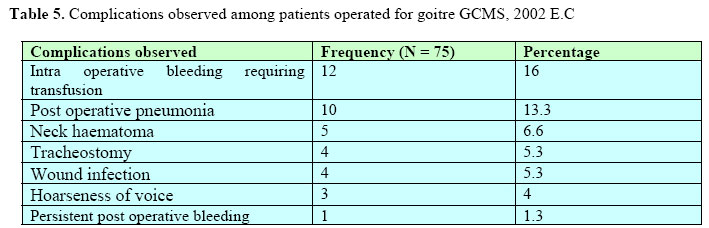
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 21-27 Goitre in a Teaching Hospital in North Western EthiopiaAbebe Bekele, Mensur Osman. Department of Surgery, College of Medicine and Health Sciences, University of Gondar, Ethiopia. P.O.Box 196, Gondar Ethiopia. Code Number: js06030 Background: The endemicity of goitre in Ethiopian high lands has been well established. There are however few studies done in the country, especially the study area, on the pattern and surgical management of goitres. This study was aimed at determining the pattern and surgical management of goitres in patient seen at Gondar College of Medical Sciences (GCMS), a teaching and referral Hospital, North Western Ethiopia. Introduction Goitre is defined as enlargement of the thyroid gland that normally weighs 25-30g. The spectrum of the diseases that occur in this gland ranges from a variety of thyroid tumours, altered functional states and inflammatory conditions, to some rare forms of disorders. Goitres are reported to occur in about 4-15% of a given population world-wide1,2 3 ,. Ultrasonography results indicate that goitre could be present in as much as 30 percent1,2,3 and autopsy findings show that 50% of the general populations have goitre without clinical manifestation2 . Thyroidectomy is the most common endocrine surgery done world-wide. Operative treatment is considered standard for patients with compressive goitres. However, small non-toxic goitres have been treated with L-thyroxin, radioiodine therapy or combination of the two6,7,8 . Today, after Theodor Kocher revolutionized thyroid surgery, the mortality from this procedure is approaching zero5 . Thyroid swellings are common in Ethiopia, especially in the mountainous parts where the altitude ranges is 1,500-2,000 meters or more above sea level9,10 . Previous studies in the country have shown simple (non-toxic) nodular thyroid enlargement to be the most common variant11,12,13 . In the majority, these benign enlargements do not cause significant symptoms hence; medical attention is not often sought early (12). Thyrotoxicosis is also not uncommon among Ethiopians14 . Few studies in Ethiopia have reported the pattern of goitre11,12,13,14 . This is particularly true for the study area (North western Ethiopia) where only a single study exists (12). Hence, this study was conducted with the objective of reporting the pattern of thyroid swellings and their modes of surgical management and its outcome. Patients and Methods The study was a prospective clinical type, conducted at the Gondar College of Medical Sciences (GCMS) teaching and referral Hospital, North Western Ethiopia. The hospital is the main surgical facility for an estimate of 4.5 million people in the region. All patients admitted to the hospital between December 2003 and August 2004 for surgical treatment of goitre were included in the study. Informed consent was obtained from each patient before being included in the study. Data was collected by using pre-designed questionnaire which included socio-demographic variables, dietary history, clinical presentation, laboratory and histo-pathologic results, type of operative management, observed complications and post operative follow up. The questionnaires were filled by medical doctors who evaluated and admitted the patients. All patients were reevaluated and records counter checked by the principal investigator to assure uniform classification of cases. The size of the goitres was graded from 0-3 according to Perez et. al9. Wayne’s clinical index15 was used for clinical diagnosis of thyrotoxicosis. Pre operatively, all patients were subjected to fine needle aspiration cytological (FNAC) examination from the anterior neck mass and blood was taken for determination of thyroid function tests (TSH, T4 and T3) by using the ELISA (Enzyme linked iso-sorbent assay) method. Intra operative findings were documented by the operating surgeons. All postoperative thyroid tissues specimens removed surgically were weighed and subjected to histopathologic examination for diagnostic confirmation. All patients were followed until discharge. The data was then compiled and entered to a computer. Analysis was made using statistical package EP-INFO-VER-6. Results A total of 80 patients were admitted to the hospital for surgical management of goitre during the study period. Majority of the patients (82.5%) were females (F: M = 4.7:1). The mean age at presentation was 35.7 years (SD= 13.71), the age range being 13-68. The peak incidence was at the third and fourth decade of life, 41.2% and 33.7% respectively. Cabbage was not commonly used as regular diet in 70.0% and only five patients (6.3%) had knowledge of their table salt to contain iodine. Endemicity of goitre was reported by half of the patients and at least one family member with the same illness was reported in 26.3% of the patients. The duration of illness found to be usually long. The mean duration at presentation was 8.8 years, (range being 3 months to 40 years). One particular patient presented 40 years after the onset. Forty percent of the females reported rapid growth of the neck mass during late pregnancy and labour. Prior to admission, Lugol's iodine was prescribed elsewhere for 12 patients and 11(13.8%) attended traditional medicine, with very little reported clinical response. Three (3.75%) had previous thyroidectomy, and 2(2.5%) were treated medically for thyrotoxicosis. Desire to have the huge neck mass removed for cosmetic reasons, significant respiratory obstructive symptoms and rapid growth of the silent mass were the leading reasons for visiting the hospital by 27(33.8%), 21(26.3%) and 10(12.5%) of the patients respectively. Stigmatization by the community such as repeated insult, seclusion from the community and feeling of shame were also contributing social reasons for medical consultation. (Table 1) The thyroid gland size at admission was grade III in nearly 80% of cases. All lobes were enlarged in 70.0% of the cases while 25% had either one of the lobes enlarged. Solitary thyroid nodule was detected in 5% cases (Table 2). (Table 3) Eighty percent of the patients had benign goitres, either diffuse, multi nodular or thyroid cysts. A diagnosis of malignant goitre was made clinically in nine patients (11.3%) and was confirmed by histopathology. Follicular and papillary carcinomas were the leading variants in 44.4% and 33.3% of the malignant cases respectively. There were 2(2.6%) cases of Hurtle cell adenoma. Five patients had hyperthyroidism which was confirmed biochemically. Except one patient with anaplastic carcinoma which was found hypothyroid, the remaining 74 patients were euthyroid. The commonest indication for surgery was for cosmetic reason. All benign cases were treated by bilateral sub total thyroidectomy and lobectomy in 66.6% and 29.3% cases respectively. Five of the patients with thyroid cancer had inoperable advanced malignancy, hence, only supportive therapy was provided. Isolated right lobectomy, total thyroidectomy with lymph node dissection and simple debulking were done in the operable cases.(Table 4). The mean duration of surgery was 72.5 minutes (Range=30-145 minutes) and the mean weight of thyroid tissue removed was 320 grams (Range=20-1200 grams). Significant intraoperative bleeding requiring blood transfusion was encountered in twelve (16%) operations. Eight patients were given one unit, three patients required two units and one patient required 3 units of blood. Six patients, four of whom (5.3%) required tracheostomy, developed airway obstruction due to tracheal collapse. Post operative bleeding with expanding haematoma in the neck was encountered in one patient who had to be re-explored within 24 hours. During the postoperative period, pneumonia was the commonest complication observed in 13.3% of the patients. Three patients (4%) developed mild hoarseness of voice. Seventy-two (70%) of the patients were discharged improved after mean duration of hospital stay of 14.1 days. The range of hospital stay was 2-38 days. Five were discharged un-operated with the same condition. Three patients died (Table 5) Anaplastic and mixed anaplastic-follicular carcinomas were seen in one patient each. Metastasis to the cervical lymph nodes was predominantly seen in the papillary while distant metastasis, either to the chest, skull, pelvic bones and shoulder, was seen in the Discussion Simple goitre was reported to be very common by many studies in Asia, Middle East, Far East, other African countries and Ethiopia4,11,12,13,16,17. The results of this study are in consistence to findings from other studies. The ages of our patients are similar with the above studies, but the female to male ratio was lower than studies done in Vietnam (9:1) and Nigeria (8.6:1). Although thyroid swellings are said to be common in females, the results of our study might be explained by an increased occurrence of goitre in both sexes due to high goitre prevalence. The tendency of men to visit health institutions when sick more than the female might hide the true sex predominance. We have found that our patients knew very little about goitres. Only 30% know that iodine deficiency is the cause of endemic goitre. The remaining think that alcoholism and drinking bad water from a river cause this disease. Twelve and a half percent thought it was contagious from relatives and neighbours. Delayed presentation for treatment is still a common feature in most patients. The absence of symptoms besides the bulky mass might be the most probable reason for this. Hospital visits are also found to be determined by cosmetic interest, educational status, distance from health facilities, recent onset of new symptoms, and psychosocial trauma and stigmatization the patients suffered because of their illness. A report from the same institution had previously shown a high rate of thyroid cancers in Gondar12. Similar results have been found in this study where 11.3% of the patients had a histologically proven thyroid malignancy. The rate of cancer in our series was very high when compared to findings of 1.8% in Addis Ababa11, 4% in Nigeria16, 2.8% in Vietnam17 and 8.4% in South west Thames18. The follicular type of thyroid cancer was the commonest variant. This might be because follicular carcinoma is said to arise from a long standing simple goitres, which are very common in Ethiopia. It is interesting to note that 7 (77.7%) of the thyroid cancer patients and all of those with follicular carcinoma had a blood group of O+. We have also found that 46 (57.5%) of all the patients with goitres had blood group of O+. Whether blood group O+ is a risk factor for the development of goitres, especially follicular carcinoma or the finding is a mere coincidence needs to be proven. with follicular carcinoma had a blood group of O+. We have also found that 46 (57.5%) of all the patients with goitres had blood group of O+. Whether blood group O+ is a risk factor for the development of goitres, especially follicular carcinoma or the finding is a mere coincidence needs to be proven. All our patients were subjected to FNAC examination and all post operative specimens were sent for histopathological conformation of the diagnosis. FNAC of the thyroid gland is a rapid, minimally invasive first line procedure in the evaluation of a thyroid swelling3,4,5. The main controversy lies in the diagnosis of patients with follicular neoplasia, the diagnosis of a carcinoma being made only by histopathological examination of the postoperative specimens3. In our study, 62 (96.9%) of the 64 of the simple goitres were accurately diagnosed as simple goitres by FNAC. One patient diagnosed as a follicular neoplasia by FNAC was found to be simple goitre after surgery. One patient diagnosed as simple multinodular goitre by FNAC was found to have multiple foci of toxicity. There were eight swellings reported as follicular neoplasia by FNAC. Biopsy confirmed that two were hurtle cell adenoma, one was a mixed follicular-anaplastic carcinoma, and four were follicular carcinoma. The remaining one was a simple goitre. All the papillary and anaplastic carcinomas were accurately diagnosed by FNAC. We have found FNAC to be easily performed, cost effective and a relatively accurate diagnostic tool. Therefore, strongly recommend its routine use as a first line investigation in patients with goitre. Routine determination of the thyroid hormone levels for all cases of goitre was found not to be important. Five (6.25%) of the patients had Wayne’s clinical index scores above 27; all were biochemically hyperthyroid. One patient with an equivocal Wayne’s index score of 16 had serum hormone level within the normal range. Except the patient with advanced anaplastic carcinoma who was biochemically hypothyroid, all the remaining patients had Wayne’s score below 7 and all were biochemically euthyroid. Wayne’s index was found to be a very useful clinical indicator of hyperthyroidism if appropriately used. Based on this, routine determination of serum hormone level for all patients’ with goitre, especially in health facilities where this test is scarcely available and expensive may be done without. This expensive test should only be mandatory in those with definitely toxic or equivocal Wayne’s score. Surgical treatment is considered standard therapy for patients with large, compressive multi nodular goitres5,6. However, although thyroid surgery leads to rapid tracheal decompression in most patients, it is not with out risk. Moreover, goitres recur after surgery in 10-20% of patients6. The type of thyroid surgery done in our institution was found similar with reports from other centres11,12,16,17,. However, intra-operative complications especially bleeding are common. This is due to the presence of big bulk of the highly vascularized thyroid tissue in most of our patients and the presence of advanced thyroid malignancies6. We have also found that the duration of surgery, post operative stay and postoperative complications to be higher in patients operated for big goitres and for thyroid carcinoma. Three patients died after admission. One patient with follicular thyroid carcinoma died during the administration of general anaesthesia. Excluding this patient, mortality from thyroidectomy was 2.6%. This figure is higher than that from Vietnam (0%) and Nigeria (0%), but lower from Addis Ababa (3.2%) (12). The causes of death were severe hospital acquired pneumonia in a 40 years old patient operated for size grade III simple goitre and advanced papillary carcinoma complicated by repeated tracheostomy tube blockage in a 60 years female patient. The over all hospital stay of patients was high. Since most of our patients are poor people from very far distance from the hospital, it is customary to admit all patients for surgery at their first visit. This adds to the long preoperative stay due to long operation waiting list and time required for patient preparation. The occurrences of post operative complications are responsible for post operative longer stay. Conclusions and recommendations
Acknowledgement We are indebted to the patients involved in the study, to the thank intern doctors of year 20022003 for their assistance during data collection and patient care, to all the surgeons, physicians, nurses and the operation room staff who were involved in the care of these patients and the Research and Publication office of the Gondar College of Medical Sciences for funding the study. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06030t4.jpg] [js06030t3.jpg] [js06030t2.jpg] [js06030t5.jpg] [js06030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}