 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
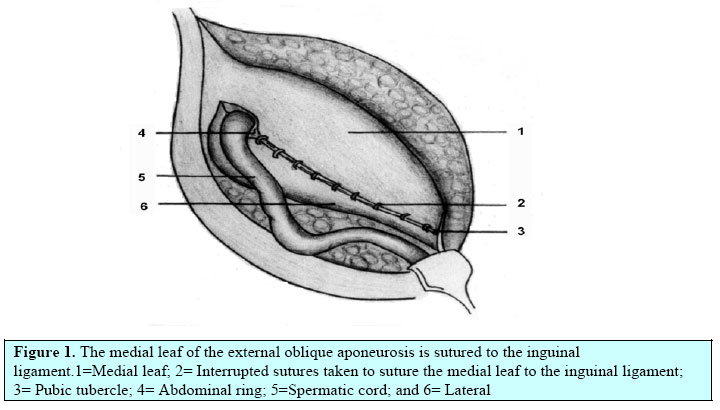
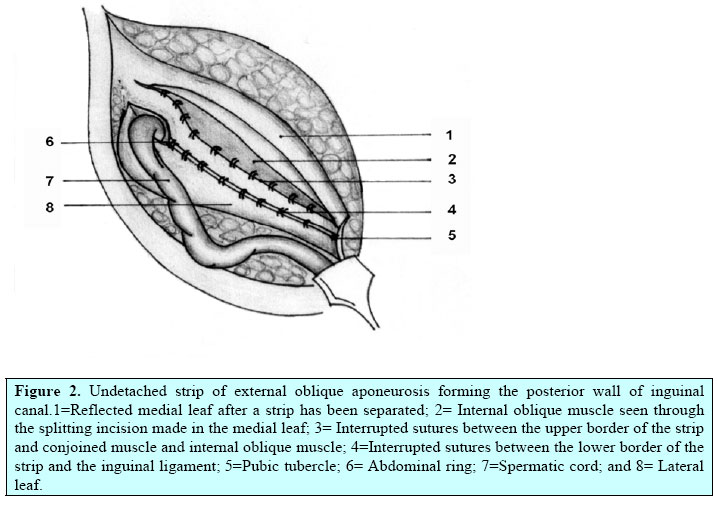
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 28-34 Comparative Study of Open Mesh Repair and Desarda’s No-Mesh Repair in a District Hospital in India M. P. Desarda1 M.S, A. Ghosh2 DNB, M.B.B.S 1Professor and Head, 2Resident in surgery, Dept of surgery, Poona Hospital & Research Centre, Pune. Code Number: js06031 Background: The first author has described a new technique of pure tissue hernia repair and published his results previously1,2. This article describes the results of a comparative study of this new technique and the open mesh repair done in a district level general hospital set up in India. Introduction Improvements in surgical technique and a better understanding of the anatomy and physiology of the inguinal canal have significantly improved outcomes for many patients. These improvements have occurred most notably in centers specializing in hernia surgery, with some institutions reporting failure rates of less than 1%3,4 . In contrast, failure rates for general surgeons, without expertise in hernia surgery, or the nonconsultant staffs, operating in smaller district level general hospitals remain significantly higher (up to 10% for primary hernias and 5% to 35% for recurrent hernias5 . This has important socioeconomic implications, adding an enormous cost of treating the condition, which runs into billions of dollars. Success of groin hernia repair is measured primarily by the permanence of the operation, fewest complications, minimal costs, and earliest return to normal activities. The search for a method that accomplishes all the above goals in the hands of non-consultant staff continues. Publication of the results of the author’s series of operation prompted many others to adopt this technique1 . Their results, as communicated to the author, are equally encouraging. This study is undertaken in a district level general hospital which is not a specialized hernia centre to compare the early and late morbidity as seen with the author’s technique and the mesh repair done by general surgeons who are not labeled as expert hernia surgeons and are not doing only hernia surgery. Methods This was a retrospective study of 203 cases with 225 inguinal hernias repaired by open mesh repair and 252 cases having 269 inguinal hernias repaired by the author’s technique from April 1998 to December 2003. All the surgeries were performed at Poona Hospital and Research Centre, a district level multidisciplinary general hospital. Patients admitted in unit1 were operated by the author’s technique and patients admitted in unit 2 were operated by mesh repair. None of those surgeons were specialist in hernia surgery. Only those patients between 20 to 80 years of age and those operated under spinal or local anesthesia were included in this study. Exclusion criteria included associated surgical pathologies where the patient was getting operated for both conditions at the same time, laparoscopic repairs or the patients given general anesthesia for any reason. The data was collected as regards hospital stay, pain, ambulation and complications recorded during operation or the hospital stay. Pain was measured as mild pain (no analgesics), moderate pain (oral analgesics) and severe pain (parenteral analgesic). Ambulation was measured as limited movements inside the room, free movements as movements out side the room and no movements where bed rest was advised. Follow up record was collected from the out patient record of the respective units till December 2005 and the data of pain, infection or other complications were recorded. 32 patients in mesh group and 18 patients in authors group, whose follow up was seen to have been lost in the record were called back to the clinic for examination by the operating surgeon or his resident surgeon. But, none of them have turned up for the follow up. Thus, 234 (92.8%) patients in the author’s group and 171(84.3%) patients in the mesh group were followed up for a median follow up period of 4.1 and 3.9 years respectively (Range 1-5 years).Appearance of a bulge with cough impulse was treated as recurrence. Use of short form 36 was done. Data was analyzed using the Statistical Program for Social Sciences (SPSS 7.5.1 for Windows) package. The statistical methods used to compare the two data were the chi square test and the independent sample t test. The operative technique of this new repair method was followed as described by Desarda2 and mesh repair was followed as described by Lichtenstein and Amid6. The Ethics Committee of the hospital cleared the study. Desarda’s Repair Technique. Skin and fascia are incised through a regular oblique inguinal incision to expose the external oblique aponeurosis. The thin, filmy fascial layer covering it is kept undisturbed as far as possible and an assessment made about the strength of it and its thinned-out portion. The thinned out portion is usually seen at the top of the hernia swelling, extending and fanning out to the lower crux of the superficial ring. The external oblique is cut in line with the upper crux of the superficial ring, which leaves the thinned out portion in the lower leaf so a good strip can be taken from the upper leaf. The external oblique, which is thinned out as a result of aging or long standing large hernias, can also be used for repair if it is able to hold the interrupted sutures. The cremasteric muscle is incised for the herniotomy and the spermatic cord together with the cremasteric muscle is separated from the inguinal floor. The sac is excised in all cases except in small direct hernias where it is inverted. The medial leaf of the external oblique aponeurosis is sutured with the inguinal ligament from the pubic tubercle to the abdominal ring using 1/0 monofilament polyamide (Ethilon) or polypropylene (Prolene) interrupted sutures. The first two sutures are taken in the anterior rectus sheath where it joins the external oblique aponeurosis. The last suture is taken so as to narrow the abdominal ring sufficiently without constricting the spermatic cord (Figure 1). Each suture is passed first through the inguinal ligament, then the transversalis fascia, and then the external oblique. The index finger of the left hand is used to protect the femoral vessels and retract the cord structures laterally while taking lateral sutures. A splitting incision is made in this sutured medial leaf, partially separating a strip with a width equivalent to the gap between the muscle arch and the inguinal ligament but not more than 2 cms. This splitting incision is extended medially up to the pubic symphysis and laterally 1–2 cms beyond the abdominal ring. The medial insertion and lateral continuation of this strip is kept intact. A strip of the external oblique, is now available, the lower border of which is already sutured to the inguinal ligament. The upper free border of the strip is now sutured to the internal oblique or conjoined muscle lying close to it with 1/0 monofilament polyamide or polypropylene interrupted sutures throughout its length (Figure 2). The aponeurotic portion of the internal oblique muscle is used for suturing to this strip wherever and whenever possible to avoid tension; otherwise, it is not a must for the success of the operation. This will result in the strip of the external oblique being placed behind the cord to form a new posterior wall of the inguinal canal. Table 1. Table shows comparison of new method with international studies of open mesh repair
At this stage the patient is asked to cough and the increased tension on the strip exerted by the external oblique to support the weakened internal oblique and transversus abdominis is clearly visible. The increased tension exerted by the external oblique muscle is the essence of this operation. The spermatic cord is placed in the inguinal canal and the lateral leaf of the external oblique is sutured to the newly formed medial leaf of the external oblique in front of the cord, as usual, again using 1/0 monofilament polyamide or polypropylene interrupted sutures. Undermining of the newly formed medial leaf on both of its surfaces facilitate its approximation to the lateral leaf. The first stitch is taken between the lateral corner of the splitting incision and lateral leaf of the external oblique. This is followed by closure of the superficial fascia and the skin as usual. Results In the authors group of 252 patients, 62 were direct, 104 indirect, 5 pantaloon, 53 recurrent, 11 obstructed and 17 bilateral hernias. In the mesh group of 203 patients, 62 were direct, 96 indirect, 11 pantaloon, 6 recurrent, 7 obstructed and 22 bilateral hernias. The mean age of the patients in the mesh group was 54.29+/14.64years while in the author’s technique it was 51.55+/-16.35 years. 28 patients in the author’s technique and 26 patients in the mesh group had a co morbid condition. There was no significant difference in the age and the co morbid condition in both the groups (p>0.05). The mean stay in the author’s technique was 1.22+/-0.89 days while it was 3.59+/-1.93 days in the mesh group. This difference is highly significant (p<0.001). The mean time to return to work in the author’s technique was 8.48+/ 2.43 days while it was 12.46+/-2.11 days in the mesh group. This difference is also highly significant (p<0.001). There were 5 complications in the author’s technique while there were 16 complications in the mesh group. This difference in complication rates is also highly significant (p=0.003). There was no recurrence seen with the author’s technique while there were 4 recurrences in the mesh group (1.97%). In addition there were 3 patients in the mesh group who underwent reoperation for chronic debilating groin pain (1.47%). Thus the total reoperation rate in the mesh group was 7/203 (3.44%). No patient had discomfort for more than 15 days in the author’s technique, where as, in the mesh group, 4 patients had moderate pain and 15 patients had mild pain or discomfort at the end of 1 month; 2 patients had moderate pain while 14 patients had mild pain/ discomfort at the end of 6 month and 13 patients continued to have mild pain or discomfort at the end of 1 year. Thus at the end of 1 year there were 13 (6.4%) out of 203 patients who had chronic groin pain in the mesh group while there was no incidence of chronic groin pain in the author’s technique. Discussion Inguinal hernia is a very common condition afflicting mankind. Newer techniques are developed as the complication rate of older ones become unacceptable. The Lichtenstein technique and its modifications are widely practiced in the world but their complication rates and failures are more in the hands of non-consultant staff. Mesh repair, plug repair, plug and mesh repair or recently introduced PHS have all confused what is best and what to follow in the minds of such surgeons, who are not expert in hernia surgery. This necessitates the introduction of a new technique of hernia repair with reduced complication rates in the hands of such general surgeons or the non-consultant staff operating at smaller or district level general hospitals. In this present study of 455 patients, the new method of hernia repair described by the first author seems to be superior to the open mesh (Lichtenstein) method on many counts. Both the groups are statistically similar with regards to age, sex, and co morbid conditions. The post operative stay, time taken to ambulate the patient and the time taken for the patient to return to work are all significantly less in the new method compared to the Lichtenstein method. Also the postoperative pain and rate of complications is lesser with the new method. In the new group there are no recurrences or re-surgeries required. There were four recurrences and three re-explorations due to chronic severe groin pain in the mesh group making a total of 7 (3.44%) who had re-operation. All the re-surgeries showed extensive fibrosis reaction in the inguinal canal due to the foreign body reaction of the mesh. In both the patients who were explored for chronic debilitating groin pain, the spermatic cord was seen to be enmeshed in the strong fibrous tissue around the mesh. Careful dissection and release of cord from the extensive adhesions was required. Thus it can be inferred that the strong foreign body fibrous reaction seen with mesh repair is responsible in spermatic cord and nerve enmeshment leading to chronic groin pain. The new technique being a pure tissue repair will not cause extensive fibrosis as seen in mesh repair. Some studies reported chronic groin pain following open mesh repair in 28.7 %( 7) to 43.3%. (8) This study also shows chronic groin pain in the postoperative period in the mesh group in 18 % of cases. 1.47 %( 3 patients) had to be re-explored for severe groin pain. In contrast, there was no incidence of chronic groin pain in the new method. Chronic groin pain affects the quality of life of the patients. Since quality of life is a very important consideration after any surgery this new method seems to score over the Lichtenstein technique on this count also. This new technique of inguinal hernia repair is easy to learn and does not require complicated dissection. As the steps in this surgery are fixed there is very less scope for modification by individual surgeon. Hence even in the hand of junior surgeons this technique will prove to be very effective. As against this individual surgeons bring in a lot of modification in the Lichtenstein repair (like using a smaller size mesh or not overlapping the mesh over the tissues adequately). These modifications add to the failure rates in the Lichtenstein repair. Moreover, the new technique of hernia repair does not need any costly mesh or laparoscopic instruments. This makes this repair highly cost effective. A cost effective repair that gives excellent results will go a long way in reducing health care cost in those days of cost ergonomics. This new method of hernia repair described by Desarda is based on physiological principle. The posterior wall of the canal is made up of the transversalis fascia, which is strengthened medially by the falx inguinalis or edge of rectus and more laterally by the aponeurotic extensions from the transversus abdominis arch that make the posterior wall strong. But these aponeurotic extensions are absent or deficient in 53% of the population9. Strong musculo-aponeurotic structures around the inguinal canal still give protection to prevent the herniation in such individuals. This protection is lost if those muscles are weak. The weak and physiologically a-dynamic posterior wall of inguinal canal in such individuals leads to hernia formation1, 2. Bassini/Shouldice or similar open repairs use those muscles for repair even if they are weak leading to failures. The strip of external oblique aponeurosis provides the aponeurotic element to the transversalis fascia of the posterior wall. Actions like coughing, crying and straining cause contraction of the abdominal muscles. Contraction of the external oblique muscle creates lateral tension in this strip while contraction of the internal oblique/conjoined muscle pulls this strip upwards and laterally, creating tension above and laterally, making the strip a shield to prevent any herniation. The strip provides a new insertion to the weak and flabby internal oblique and transversus abdominis. This helps to improve the muscle contractions of the internal oblique and the transversus abdominis muscles. The additional strength given by the external oblique muscle to the weakened conjoined muscle to create tension in the strip and prevent hernia recurrence is the essence of this operation1,2. Tension created in this strip is graded as per the force of muscle contractions. Stronger intra abdominal blows result in stronger abdominal muscle contractions and stronger muscle contractions result in increased tension in this strip to give graded protection. The strip or the suture line is without any tension at rest. Thus, a strong and physiologically dynamic posterior wall is prepared in this operation1, 2. As this new technique of inguinal hernia repair compares favourably with other methods of hernia repair, this technique needs to be used more extensively. Comparison with International Studies. The data of the Lichtenstein group in our study may not match with the data of international studies. Hence the data of this new technique was compared with the data of international studies of open mesh repair (Table 1)
The results of the new repair described by the author look very promising. Large-scale long-term multi-centric trials need to be conducted to evaluate this repair further and establish this repair among the general population of surgeons. This repair is easy to learn with minimal complications or recurrence. This operation is based on the physiological principles and this concept of physiological repair of inguinal hernia needs to be studied. Conclusion The results of the new repair described by the author look very promising. Large-scale long-term multi-centric trials need to be conducted to evaluate this repair further and establish this repair among the general population of surgeons. This repair is easy to learn with minimal complications or recurrence. This operation is based on the physiological principles and this concept of physiological repair of inguinal hernia needs to be studied. This new repair has the potential to become the gold standard of hernia repair in years to come. Acknowledgement. Since its first publication in 2001, the author has received communication from the following surgeons in Poland, Cuba, Korea, Albania, Libiya, Ukraine, Iran, Brazil and India of clinical trials being conducted by them that had shown similar results without recurrence till date. They are:
Others were who showed interest in procedure included:
To all of them the principal author is very grateful References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06031f1.jpg] [js06031f2.jpg] |
| |||||||||

{kind=link}
{kind=link}