 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
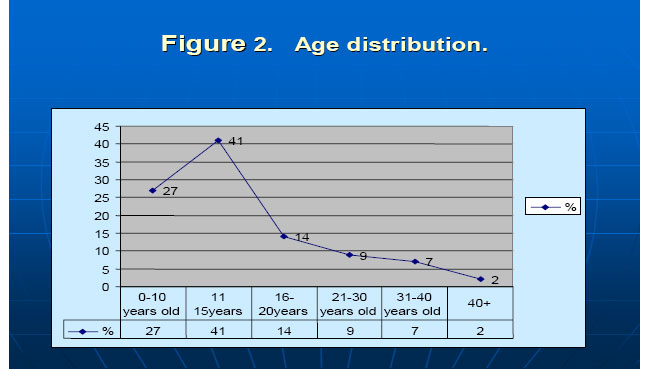
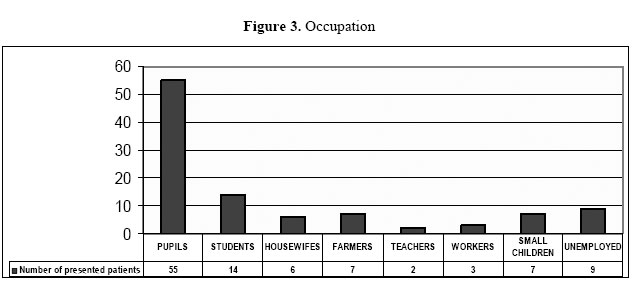
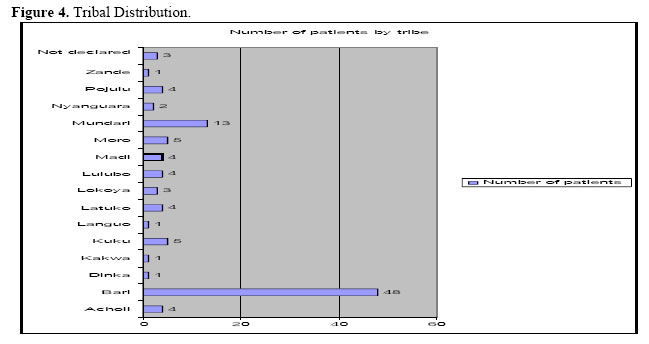
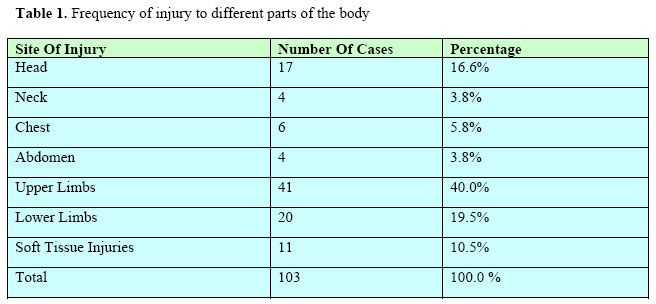
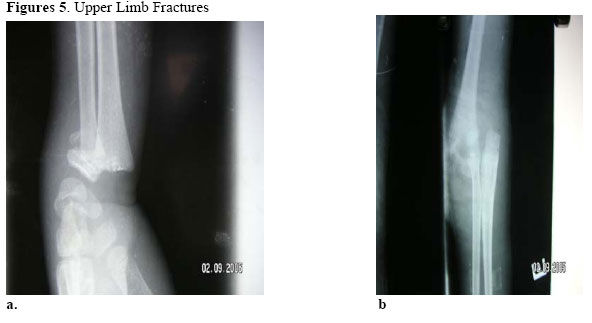
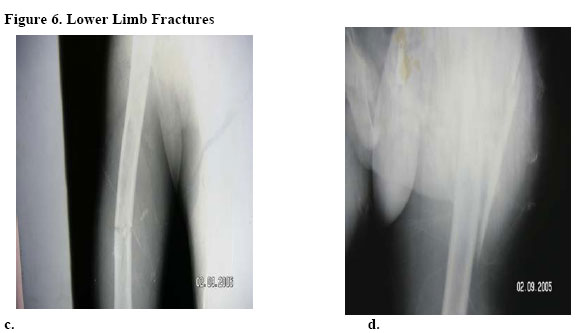
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 35-40 Patterns of Mango Tree Trauma in Juba Teaching Hospital Dario Kuron Lado, MBBS, FS SMSB, Surgeon - Juba Teaching Hospital, South Sudan. Telephone: (249) 122151736 / (249)820050. Email: kuronlado@yahoo.com Code Number: js06032 Background: Mango trees constitute a third of all the trees in Juba Town and peri-urban area and they produce fruits twice every year. This study was aimed at analyzing patterns of injury in mango tree trauma and evaluating the severity of injuries sustained. Introduction Juba Teaching Hospital established back in the early 1920s is a Central Hospital in the Southern Sudan. The hospital serves all the population of equatorial provinces and during peace time it serves all Southern Sudan people. During the war, the standard of care in the hospital was drastically affected to the point that it was impossible to render minimum services to the people, leave alone the pressing number of war injured people. Fortunately, the international community took the initiative to directly support and help the people of Juba, particularly by strongly backing up the services in Juba Teaching Hospital. Now that peace is achieved, the hospital, like the people and everything in the south, including Juba Town itself, is trying to recover and to prepare for challenges of peace. As we all know, peace brings with it new issues and new health problems. The first is the increasing population of the town; others include appearance or diseases associated with free traveling from the neighboring countries, diseases like Ebola, yellow fever and most importantly HIV. During the peaceful period, we are looking forward to develop our area in terms of infrastructure, roads and bridges, but these may pose a new challenge of road traffic accidents when there are good tarmac roads to the extent that traffic regulation becomes more difficult. Is there too much civilian violence, so that we need police empowerment? Do we have careless drivers on the streets? Do we need to pass a law ordering the constant use of safety belts and helmets etc? These will be some of the questions to ask and get answers to in the nearest future. After all this recital, I do want to suggest that during mango fruit season, there are as many children sustaining trauma to the limbs and different parts of the body as there are patients injured elsewhere during RTA. So it occurred to me that perhaps this mechanism of trauma will add to our health problems, and a burden which needs to be explored and examined with the aim of prevention. The aims of this study were to examine the different patterns of injury in mango tree falls, to evaluate the severity of injuries sustained, to assess management lines and to find possible preventive measures. Methods In this study, 103 patients who sustained mango tree injuries were evaluated. The patients’ ages, sex, tribe and nature of injury sustained after falling from mango trees (Figure 1) were recorded and analysed. Results Of the 103 patients reviewed, 80 were males and 23 females (Male:female ratio = 3.5:1). The majority of patients were children; those aged 11-15 years constituted 42%, followed by those of 10 years and below who contributed 28% (Figure 2). The children were mostly school pupils. All the tribes living in Juba town were represented in different percentages, but the Bari and Bari-speaking tribes constituted the majority, 48% and 25% respectively (Figures 3 and 4). Most injuries were in the limbs (60%) with the upper limbs dominating (40%) compared to the lower limbs (20%) (Table 1). The most serious injuries sustained by the patients in this study, included splenic rapture (3 patients), severe head injury (3 patients) and spinal injury (2 patients). One patient died of severe head injury, one patient had post traumatic epilepsy and the patients with spinal injury were discharged from the hospital on wheel chair. Deformities due to long bones fractures and dislocations were rare. Discussion Mango trees constitute a third of all the trees in Juba Town and surroundings and they produce fruits twice every year. During the long war when food supply was limited and everything had to be brought in by planes, the daily main food was only mangoes. In this study the majority of the victims were children and this may be due to inexperience, as much care is needed in climbing up the mango tree and that children are careless while up the tree. Most of the mango plantation is owned by the Bari tribe and that is why this tribe was the predominate tribe in this study. The predominance of males can be explained by the social law that women are not supposed to climb a tree of any sort. As revealed in the study, mango tree injury is a phenomenon which we can compare to a traffic road injuries, where the pattern of injury is not predictable or reproducible, as this depends on the nature of the impact and its severity. The height of the tree is one factor that determines how serious the injury could be, as well as the point of impact with the ground. In this study limbs fractures formed 60 % of the injuries, most were flexion types of injury with the upper limbs forming the majority, for the common reason that when one falls, one always tries to protect the rest of the body by stretching the arm to reach the ground first, thus all the forces are transmitted through the upper limbs bones, which may not be strong enough to withstand the stress. abdominal injuries were rare but serious and occurred in 4 children. In this study, laparotomy and splenectomy had to be undertaken to save the patients’ lives. We also observed in this study that deformities resulting from limbs injuries were rare, and this could be because most victims were children. Despite the severity of injury they sustained, their healing and remodeling powers are great for long bones fractures. For the mango tree head and spinal injuries, these always pose challenging management problems, as some of these patients may need special care and rehabilitation units, the reality which is still not possible in this war torn town. The low mortality is due to predominance of limbs injuries, contrary to road traffic crushes in which head, neck and abdominal injuries are common. Conclusion „ Mango tree trauma is not a new problem, but one that is not attended to, but is attracting the attention of medical care takers because of the attendant increasing number of victims. „ The phenomenon is comparable to road traffic crushes with unpredictable patterns of injury, but some of the injuries, like the head, chest, spinal and abdominal injuries can be fatal or incapacitating. Recommendations
Acknowledgements: This work was inspired by one member of ICRC, war surgeon and urologist, Dr. Yuka, to whom I am indebted. The historical background and organizational information was offered freely by Mr. Sallyi L Samuel, the medical director of Juba Teaching Hospital. I thank him for his invaluable cooperation. My sincere regards I register to my house officers who helped in making the initial assessment of all my patients in this work. Lastly but not least, I would like to thank Mrs. Edith for typing the manuscript and doing all the computing work. Mango trees constitute a third of all the trees in Juba Town and surroundings and they produce fruits twice every year. During the long war when food supply was limited and everything had to be brought in by planes, the daily main food was only mangoes. In this study the majority of the victims were children and this may be due to inexperience, as much care is needed in climbing up the mango tree and that children are careless while up the tree. Most of the mango plantation is owned by the Bari tribe and that is why this tribe was the predominate tribe in this study. The predominance of males can be explained by the social law that women are not supposed to climb a tree of any sort. As revealed in the study, mango tree injury is a phenomenon which we can compare to a traffic road injuries, where the pattern of injury is not predictable or reproducible, as this depends on the nature of the impact and its severity. The height of the tree is one factor that determines how serious the injury could be, as well as the point of impact with the ground. In this study limbs fractures formed 60 % of the injuries, most were flexion types of injury with the upper limbs forming the majority, for the common reason that when one falls, one always tries to protect the rest of the body by stretching the arm to reach the ground first, thus all the forces are transmitted through the upper limbs bones, which may not be strong enough to withstand the stress. Compared to traffic road trauma, blunt abdominal injuries were rare but serious and occurred in 4 children. In this study, laparotomy and splenectomy had to be undertaken to save the patients’ lives. We also observed in this study that deformities resulting from limbs injuries were rare, and this could be because most victims were children. Despite the severity of injury they sustained, their healing and remodeling powers are great for long bones fractures. For the mango tree head and spinal injuries, these always pose challenging management problems, as some of these patients may need special care and rehabilitation units, the reality which is still not possible in this war torn town. The low mortality is due to predominance of limbs injuries, contrary to road traffic crushes in which head, neck and abdominal injuries are common. Conclusion „ Mango tree trauma is not a new problem, but one that is not attended to, but is attracting the attention of medical care takers because of the attendant increasing number of victims. „ The phenomenon is comparable to road traffic crushes with unpredictable patterns of injury, but some of the injuries, like the head, chest, spinal and abdominal injuries can be fatal or incapacitating. Recommendations
Acknowledgements: This work was inspired by one member of ICRC, war surgeon and urologist, Dr. Yuka, to whom I am indebted. The historical background and organizational information was offered freely by Mr. Sallyi L Samuel, the medical director of Juba Teaching Hospital. I thank him for his invaluable cooperation. My sincere regards I register to my house officers who helped in making the initial assessment of all my patients in this work. Lastly but not least, I would like to thank Mrs. Edith for typing the manuscript and doing all the computing work. © 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06032f4.jpg] [js06032f6.jpg] [js06032f5.jpg] [js06032t1.jpg] [js06032f3.jpg] [js06032f2.jpg] [js06032f7.jpg] [js06032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}