 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
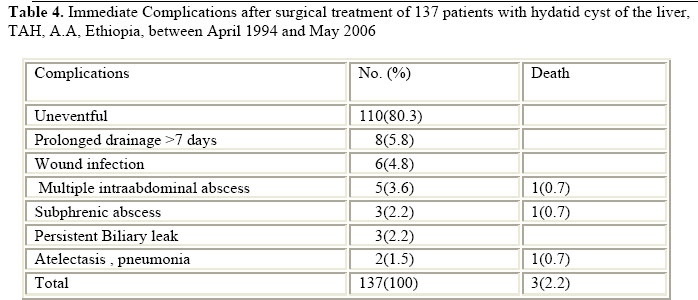
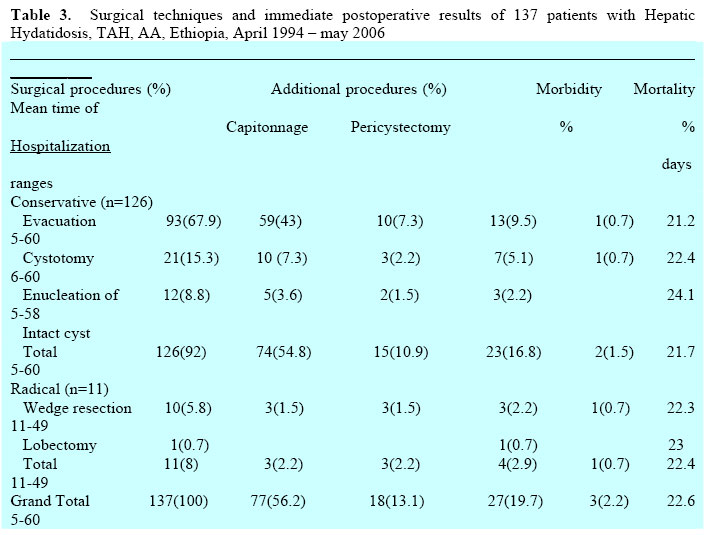
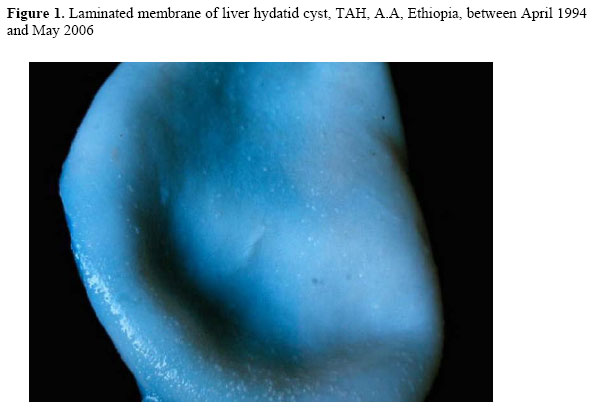
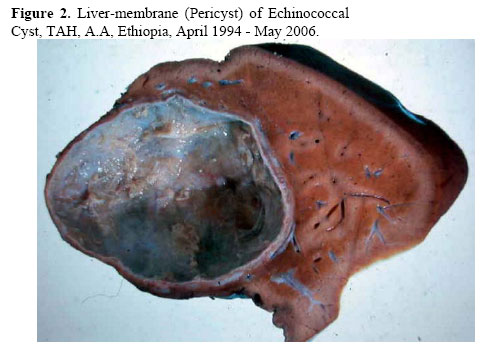
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 54-60 Hydatid disease of the liver: A 12 year experience of surgical management Hagos Biluts, Mesfin Minas, Abebe Bekele Correspondence to: Dr Hagos Biluts, Tikur Anbessa Hospital, P.O.Box 9086, Addis Ababa, Ethiopia E-mail: hagosisnow@yahoo.com, surgery@ethionet. Code Number: js06035 Objective: Information about hydatid cyst disease in Ethiopia is scarce. This study was aimed at reviewing the clinical presentations, modes of surgical management and post-operative course of patients with hepatic hydatidosis in Tikur Anbessa hospital, Introduction Hydatid disease, also known as echinococcosis or hydatidosis, is caused by infection with larval (metacestode) stage of the tapeworms of the genus Echinococcus (1, 2). Hydatidosis is still endemic in sheepherding areas of the world and is a public health problem in Mediterranean, Middle East, Asia, South America and Africa, including Ethiopia (3-8). Human infection with Echinococcus granulosis or Echinococcus multilocularis typically results in a slowly growing parasitic disease, most frequently seen in the liver in 52-77% of cases (9, 10). Diagnosis of hydatid disease relies on epidemiologic and clinical findings; on detection of the hydatid cyst by radiology, ultrasonography, computed tomography, magnetic resonance imaging, histopathology and serology (12).The Casoni and Weinberg tests are no longer used for the diagnostic workup mainly owing to low sensitivity (13). Because there is no effective medical therapy, surgery remains the principal mode of treatment to eradicate cystic echinococcosis (11, 13-15, 20). Information concerning hydatid cyst disease is scarce from the study area. Hence, this retrospective study is conducted to review the clinical presentations, modes of surgical management and post-operative course of patients with hepatic hydatidosis in Tikur Anbessa hospital, Department of Surgery, between April 1994 and May 2006. Patients and Methods All Patients ≥13 years of age, admitted to the Tikur Anbessa hospital for surgical treatment of hepatic hydatid disease between April 1994 and May 2006 were included in the review. Operation theatre registry and patients’ medical records were reviewed to determine the initial clinical manifestation, laboratory investigations, imaging studies, types of surgical procedures used, the intraoperative findings, post-operative course and final out comes. Data were collected using structured questionnaire, and analyzed using computer based statistical software SPSS version 11.0. The spectrum of surgical procedure varies from a conservative to radical resectional procedures. Conservative procedures included the use of scolicidal agents injected into the cyst cavity before manipulation, followed by evacuation (removal of cyst after needle aspiration), cystotomy (incision in the organ parenchyma and removal of the cyst) and enucleation of intact cyst. Radical techniques consisted of hepatic resection (such as wedge resection, segmentectomy and lobectomy) with or without the use of scolicidal agents. The residual cavity was treated by capitonnage (obliteration of the residual cavity using multiple purse-string sutures from the deepest to surface level) or pericystectomy (removal of the capsule or adventitial zone). Results A small male predominance was observed, in a male: female ratio of 1.2:1. Patients’ age ranged from 13 to 67 years (mean 33.5 years), with a peak incidence between 21 to 30 years. 89(65%) patients were from the rural Ethiopia and 40% of the patients had been in frequent contact with domestic animals (such as dogs). Duration of complaints ranged between 1-120 months (mean = 20.8 months). Among the 137 patients, 115(84%) had abdominal pain and 99(72.3%) had a palpable abdominal mass. In 123 of the patients (89.8%), a palpable mass or hepatomegally was noted on physical examination (Table I). Preoperative laboratory tests were of minimal diagnostic value. Ultrasonography and computed tomography were the usual preoperative diagnostic imaging procedures in 121(91.2%) and 32(94.1%) patients respectively (Table II). The cysts were located in the right lobe of the liver in 76 patients (55.5%) and in the left lobe in 38(27.7 %); the other 23 patients (16.8%) had bilobar involvement. Most patients (78.1%) had a solitary cyst, double in 14(10.2%), multiple in 16(11.7%). Twenty-three patients had hydatid cystic lesions in other organs in addition to hepatic hydatidosis. In twenty-one patients (15.3%), the cysts were complicated, including suppuration, calcification, and intrabiliary rupture. Twenty-seven (19.7%) patients developed Postoperative complication. Most common complications were prolonged drainage >7 days in 8(5.8 %), wound infection in 6(4.8 %) and multifocal intraabdominal abscesses in 5(3.6 %) patients (Table V). There were two deaths in the immediate postoperative period from Pneumonia and multifocal intra-abdominal collections followed by sepsis. Post operative surveillance also revealed a patient who succumbed to secondary sclerosing cholangitis after wedge resection and pericystectomy. Mean postoperative hospitalization was 22.6 days, range 5-60 days. The follow-up period ranged from 1 to 30 months (mean 5 months) with visits to outpatient surgical referral clinic. Recurrent disease was detected in 4 (2.9%) patients between 6 and 18 months (mean 13.5). Albendazole treatment was administered in 106 patients (77.4%), pre-operatively in patients with multiple hepatic cysts, additional organ involvement, and huge hepatic cysts likely to rupture during operation; and postoperatively as adjuvant treatment of cysts that has ruptured during operation. Intraoperatively, scolicidal agents were used in 124(90.5%) patients. The tissue surrounding the hydatid cyst is protected with sponges soaked in 2% formalin solution or rarely 70% alcohol. The cyst is then punctured and aspirated before being filled with formalin or alcohol for 5 minutes. This maneuver reduces the internal pressure of the cyst, sterilizes the cystic content, and makes the subsequent steps of surgery easier. The surgical approach was abdominal (laparotomy) in 122(89.1%) patients, one- stage thoracoabdominal in 8(5.8%), and laparotomy and thoracotomy at interval in 7(5.1%) patients. Operative management consisted of conservative procedure in 126(92%) patients, namely evacuation in 93(67.9%), cystotomy in 21(15.3%), enucleation of intact cyst in 12(8.8%) patients. Radical procedure was done in 11(8%) patients, wedge resection in 10(5.8) patients, and lobectomy in only 1(0.7%) patient (Table III). Fig I and II shows laminated membrane and pericyst (adventitial zone) of liver hydatid cyst respectively. Table 1. Initial Clinical Manifestation of 137 Patients With Hydatid Disease of the Liver, TAH, A.A, E
Table 2. Results of Diagnostic imaging studies in137 patients with hydatid disease of the liver, TAH, A.A, Ethiopia, between April 1994 and May 2006
Discussion Hepatic echinococcosis is common in sheepherding areas of the world, including Ethiopia, where it is particularly common in the rural population and at an early age 3,4,17,18. The disease should be suspected in patients who reside in sheep raising regions and have abdominal pain and hepatomegaly or palpable hepatic mass3. Hepatic hydatid cysts can remain asymptomatic for many years and then be discovered incidentally. Long duration of complaint ranging 1-120 months (mean 20.8) is in agreement with most authors10,12,17,21. Extensive preoperative laboratory tests in these patients should be limited to the base lines since our findings and those of Kevin E et al3, Langer and associates22 suggest that the results of most screening laboratory examinations are with in normal limits. We have found that computed tomography (94%) and ultrasonography (91%) are highly accurate in diagnosing hepatic hydatidosis, defining the internal structure, number, and location of the cysts and presence of complication. Our finding is in accordance with other reports that indicate the specificity of ultrasonography and computed tomography to be in the range of 90-95 % and 98% respectively3,21,22,23. Generally hepatic hydatid cysts are single, uncomplicated, and located in the right lobe of the liver3,5,24,25. Our review is in agreement with those cited in literature, where a single cyst was encountered in 107 (78.1%) cases and the disease was confined to the right lobe of the liver in 76 (55.5%) cases. Bilobar involvement as noted in 23 patients (16.8%), a pattern that reportedly occurs in 10-20 % of cases24, 26, 27. When a hydatid cyst is diagnosed, treatment should be instituted to prevent complications such as infection, calcification, cirrhosis, atrophy and rupture of cyst in to the adjacent structures, or anaphylaxis. Treatment options for cystic hydatid disease are surgery, drug therapy and percutaneous drainage. Surgery has the potential of removing the cyst, leading to complete cure6,7,13. Intra operatively, inactivation of scolices with various agents has been tried with varying success. Instillation of scolecidal agents is effective in destroying 80% to 90% of scoleces28,29. In our practice, frequently we have used 2% formalin solution and rarely 70% alcohol in a total of 124 patients (90.5%). Despite some reports, we have not encountered significant complications secondary to the use of these solutions26. The surgical procedures of choice in our experience were mainly conservative approach with removal of the germinal and laminated layers and preservation of pericyst i.e. complete excision of the disease processes with maximum preservation of tissue. This is also the experience of other authors5,6,17,30. Occasionally, cyst is removed by pericystectomy, segmentectomy or partial hepatectomy5,6,7,17. We utilized hepatic resections in 11(8%) patients, which is in agreement with Kevin and others3,5,26 who reported hepatic resection rate of 4-11%. Hepatic wedge resections are indicated only when there is atrophy of the liver or cysts situated laterally in the left lobe. The principal indications for lobectomy are large cysts involving more than half of the lobe or no salvageable parenchyma of the lobe remains, multiple unilocular cysts and sequel of hydatid disease such as suppuration, fibrosis, cirrhosis, atrophy and calcification26, 30, 31. Some advocates of radical resection approaches claim that postoperative complications, mean postoperative hospitalization and recurrence rates are decreased32,33. It is well known that using this approach, the exogenous cysts are included within the resected material, an important factor for avoiding recurrence. Despite these advantages, there is a large group of surgeons who believe that these procedures, especially liver resection, are overtreatment of a benign disease20,22,32,33. Proponents of conservative surgical procedures reported low mortality (less than 5%); a recurrence rate of less than l0% and comparable hospital stays3,5,17,35 Radical surgical intervention, however, is associated with a recurrence rate of less than 5 percentage26,27, but bleeding and persistent biliary fistulas may necessitate reoperation in as many as 6% of patients26. Although, it is difficult to compare conservative (126/137) versus radical procedures (11/137) in terms of their morbidity, mortality, and hospital stay, this review revealed that radical procedures were accompanied by high morbidity (4/11), mortality (1/11), and comparable mean time of hospital stay (22.4 versus 21.7 days). Major postoperative complication and operative mortality were seen in 27(19.7%) and 3 (2.2%) patients respectively. These finding are similar to Huguier and co-workers36, and others3-5,26,35. Mean postoperative hospitalization was 22.6 days, range 5-60. This is also in accordance to many authors3,35,36. The follow-up period ranged from 1-30 months (mean 5 months). A recurrence rate of 2.9% is acceptable compared to most surgeons3,5,26,27,35. Conclusion Hepatic echinococcosis is common in rural communities of Ethiopia, the disease should be suspected in patients who reside in sheep/cattleraising regions and have abdominal pain and hepatomegaly or palpable hepatic mass. Abdominal ultrasound should be the investigation of choice. Hepatic Hydatid cysts are benign infectious lesions that necessitate early surgical therapy to prevent complications. Complete excision of hydatid cyst(s) and procedures that conserve liver tissue are appropriate for most patients with hepatic hydatid cysts. Additional pharmacological treatment with Albendazole should be carried out for high-risk group patients. Acknowledgment. We would like to thank Professor Schneider Jacob for his help to access histophathological achieves, and all the staff members of the department of surgery for the support to conduct the study. References:
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06035f2.jpg] [js06035t4.jpg] [js06035t3.jpg] [js06035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}