 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
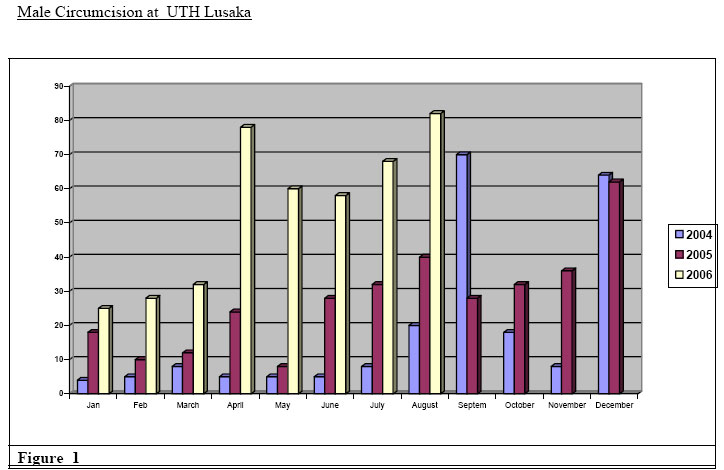
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 66-71 Male Circumcision and HIV in Zambia Kasonde Bowa1 MSc,M.Med,FRCS, Mainza Lukobo2, BSc, DrPH 1University Teaching Hospital Lusaka Zambia, 2State University of Chicago, Illinois Correspondence to: E mail Kbowa@yahoo.com Code Number: js06037 Background: Over the last 10years considerable interest has developed in male circumcision as a possible tool in reducing HIV transmission in high prevalence countries of sub-Saharan Africa. Statements from normative agencies, though cautious, have encouraged the introduction of safe hospital based circumcision practice where the demand for these services exists1. The anecdotal evidence has now been followed by one randomized control trial. The results of two further trials are awaited. In the interim , interest has grown in the question of how male circumcision can be operationalised in a real clinical setting should the two ongoing trials confirm the efficacy of male circumcision. Introduction In the mid 19th century Hutchinson proposed that male circumcision could reduce STI s2. In 1980 Arthur Fink published a letter in the New England Journal of Medicine claiming that male circumcision can reduce HIV transmission 3. Since then interest in male circumcision and its role in HIV transmission has grown. Robert Bailey and co-workers have done a systematic review of the literature on this subject 4. The ecological data shows large discrepancies in HIV prevalence regionally, sub-regionally and nationally. The key difference which has been noted is that, where male circumcision rates exceed 80% HIV prevalence is below 10%, while where circumcision rates are below 20% the prevalence of HIV is close to and often exceeds 20%5. Meta-analysis of 38 studies (mainly African) found circumcised men were less than half as likely to contract HIV. Subanalysis of 16 studies of high-risk men found circumcised men 70% less likely to contract HIV6. Ten prospective studies all suggest a reduced risk for circumcised men 4. The most impressive study was done in Rakai, Uganda among discordant couples followed up for 18 months. In this group 40 of 137 uncircumcised men sero-converted during an 18 month follow up period, while none of 50 who were circumcised sero-converted7. Biological and in-vitro studies show that the inner foreskin absorbs HIV more easily than the rest of the penile skin 8. There have been three randomized controls studies to determine the efficacy of Male Circumcision in reducing HIV transmission. Two studies in Rakai and Kisumu are on going, while the orange farm study in South Africa reported in July 2005. The orange farm study showed a protective effect of Male Circumcision of 60%. With adjustment for crossover this effect was as high as 75%. The study was stopped by the data monitoring board at 18 months and all study subjects were offered circumcision9. Zambia, a typical sub-Saharan Africa country, has a low male circumcision rate (17%) and a high HIV prevalence rate (16.5%)10. In August 2004 a dedicated Male circumcision services was started at the University Teaching Hospital in Lusaka, Zambia. The University Teaching hospital Lusaka is a 2,500 bed hospital and is the main referral centre in Zambia. It serves an national population of 10 million people and an immediate catchment area of 2.5 million in Lusaka province11. The HIV prevalence in the Lusaka province is 22%, the highest in the country12. The service was set up in the Urology outpatient section of the department of surgery with external donor support. The estimated cost of setting up this service was US $27,00013. An acceptability study done prior to this showed a high acceptability for this service14. Description The male circumcision service was set up as an integrated service. It uses the staff of the urology outpatient clinic. It provides male reproductive health services, safe sex counseling, male circumcision counseling and male circumcision. It uses the same physical site for other minor urological procedures in the outpatient clinic of the urology section. Dedicated time has been allocated for the Male Circumcision services. The services are provided every day from 14.00 to 16.00hrs in the afternoon from Monday to Friday. The service is coordinated by one of the consultant urologists in the unit. Counseling is provided by two staff nurses and a desk clerk. All staff members have been trained in male circumcision and provided by the draft World Health Organization draft training manual14. Operations are performed under local anesthesia largely by one clinical officer with the support of 2 registrars in urology and the consultant urologist in charge. The operative technique used was the dorsal slit method 15, except were penile pathology was present, in which case the sleeve technique15 was used. All adults were give local anesthesia of 2% plain lignocaine, with the exception of children under 5 years. In children under 5 years they were sedated with valium 5 to 10mgs, 1mg per kg, analgesic dose, of ketamine intravenously and 0.3 to 0.6mgs intramuscular, of atropine(to counteract the sympathomimetic effects of ketamine)16. The service is offered to any client at the cost of 3 US dollars. This is the standard cost for any minor procedure in a government hospital in Zambia. Client data was obtained using data capture sheets recommended by the draft WHO male circumcision training manual15. Pre and post circumcision written instructions are provided to all clients. HIV testing is not provided. Oral analgesia is provided and standard review protocol is done after 48hrs, 7 days, 4 weeks and 8 weeks. Any adverse events are recorded in an adverse events form. The data sheets are adapted from the Kisumu research site without significant variation. Results A total of 900 male circumcisions have been done from August 2004 to August 2006. The weekly request from people seeking male circumcision at the site is 80 per week. The site was only able to do at maximum of 20 clients per week. This is only 25% of the demand. An average of 40 procedures per month was done over the 2 years period. A progressive increase from about 20 cases per month up to the current number of 90 cases per month (figure 1). The age range was from 5 months to 96 years. The largest group, 63% were between the ages of 14 to 35years. Ninety percent of clients requested for circumcision because they considered it to be protective from STI s and possibly HIV transmission. There was good follow up for the first and second visit with over 90% of clients being reviewed. There was however a loss to follow up of 40% at 3rd visit at 4 weeks and under 20% of clients returned at 4th visit in 8 weeks. The technique used was the dorsal slit method in 90% of cases. In 10% of cases the sleeve method was used, this was done only in patients with extensive glandular and penile warts. Ninety percent of the routine adult circumcisions were done by one clinical officer trained in male circumcision. All adults circumcisions were done under local anesthesia with dorsal nerve block using 2% plain lignocaine. All children, 25% of cases were done with additional sedation. There were 27 adverse events of a total 900 circumcisions. There was a decline in adverse events from the first analysis at 6months 17, when the adverse events were at 5%. The current adverse events rate is 3%. The adverse events were mild and early. The majority occurred in the first week. By the time of the final review at 8 weeks the adverse events were down to 0.06%. The main complications noted were pain, bleeding, swelling and infection. Four patients had to be taken back for re-exploration of wound after persistent bleeding. Ninety percent of patients and parents were satisfied with the outcome of the procedure. Every 3rd week of the month the site was noted to run out of surgical gloves, lignocaine and chromic cat gat 2/0 suture. Patients were required to buy these or have their operation postponed for 2 weeks until supplies were available. Discussion There have been concerns that should the two on-going trials show that Male Circumcision reduces the risk of HIV transmission, there will be a rapid scale up of Male Circumcision as an additional public health intervention in many Sub Saharan African countries19. Concerns have been expressed about the method of introduction of this service into existing clinical services. The Male Circumcision site at UTH is an example of an integrated male circumcision service site. There has been concern that the highly supervised services seen at research sites may not translate into actual clinical practice15. The UTH service site shows an adverse event rate which is comparable to that found at the 3 research sites (figure 2). The loss to follow up after 1 month is high up to 40%. In research sites loss to follow up for the whole period is just under 15%16. This may signify good outcomes and patients feeling it unnecessary to return for further reviews. It may also signify weak counseling and low patient support at the service site than is available at a research site. This raises concerns about an increased risk during the initial 6 week healing period. Research sites show up to 10% patients at research sites engaging in sex before 6weeks 16. This will be a major challenge for service sites to overcome. No selection is made at the service site, patients with penile pathology, the old and young, both HIV positive and negative patients are all circumcised. With the careful selection at research sites, which include good hemoglobin and HIV positive status, the complication rates at the services site might be expected to be higher 8,15,17. Many studies have shown that outcome of surgery is the same for negative patients at it are for positive patients in WHO stages 1 and 218. Most of the patients would have been in stage 1 and 2 at the service site. No HIV testing is offered. The low testing levels in Zambia of between 6-15%9,11, may deter patients from seeking MC, if testing were a condition for MC. None the less it is envisaged that testing should be offered in future but MC will be offered regardless of whether the patient agrees to be tested or not. The main operators at the UTH site were mixed though the large majority of cases were done by one clinical officer. The experience of the 3 research sites and the UTH site indicates no marked variation by service provider so long as appropriate training has been given. Large scale provision of this services will not be possible by using doctors only. In Zambia 600 doctors nationwide would be unable to meet the more than 80,000 MCs required to reduce an annual 4% incidence rate by half 21. Clinical officers and other paramedics would be required. This is a cadre, who is medical assistant with 3 years of training in clinical medicine. With appropriate training the cadre can attain an acceptable level of competence in performance of this operation. The technique is varied in the three sites, but it appears the use of a single technique may be easier to learn and to teach in one site and possibly one country18. The dorsal slit method is a compromise between the simple, fast but more risky clamp method and the longer more technically demanding sleeve method. It also allows for the management of clients with pre existing phimosis 15. The integration of this service in existing services is a good model and appears to have worked well at the UTH. In this case integration was to a urology out patient section. Integration may equally be done with STI clinics, Post natal clinics, Youth Friendly services and others. The limitations are with meeting high public health numbers, the service has done 900 cases over 2yrs, anticipated figures to achieve high levels of impact would have to exceed 80,000 cases per year in Zambia with an annual incidence of 42,000 new male infections22. Other public health interventions such as PMCTC have shown low levels of uptake in Zambia at about 23%23. While vertical programs such as the national blood bank service have over 80% coverage nationwide23. The 3 research sites have also done almost 5 times as many cases over half the time because of a higher investment but also because the services were vertical or stand alone services 24, where these were integrated, this was into a private service such as orange farm9. Whether the vertical service would be required at least in some of the larger sites to meets these large numbers requires discussion. The low number of doctors in Zambia at 700 below the WHO recommendations of 1 to 5,000 would be unable to meet the demands. They are twice as many clinical officers at almost 1,200 with a better rural to urban ratio22 Various surgical techniques have been used. The complication rates are similar, the importance is then adequate training (figure 2) 24. For the service site dorsal slit method is an intermediate operation, which takes the better of the two other operations. Sleeve method which is more technical and takes longer, while the clamp method which is quicker but puts the glans penis at risk and compromises the penile skin. With poor follow up the dorsal slit appears to be a better method and provide for less stringent follow up. It is likely that loss to follow up will be a major problem at service sites. In the more peripheral centres the infection rates may be higher where literacy rates and assess to tap water may be less12. The complication rates would still be less than the quoted figures of 30% of hospital based and up to 70% for traditional circumcisions25. The key issues are good training and adequate number of cases, continual follow up and monitoring of operators. Several models of scale up can be proposed, but it may be useful to use models like the national blood transfusion service which is also a public health strategy, it is centralized with provincial satellites, this allows for efficient monitoring evaluation, training and data storage. These services are targets just under 5% of national causes HIV transmissions, which are blood and blood products. PMTCT programs targeting 1015% of national causes of HIV transmission, which is mother to child transmission. These programs have not been very successful and have only reached levels not more than 25% coverage in Zambia. This is none the less considered to have been a comparative success in the region. Conclusion Following the National AIDS conference in Toronto and the plenary session on Male Circumcision19, it is evident that Male Circumcision may soon become an additional public health strategy in the fight against HIV/AIDS particularly in sub-Saharan Africa. Countries and governments may soon be looking at how best to integrate these services in national HIV programs in a cost effective manner. The male circumcision service site at the University Teaching Hospital as a fore runner in this area may be one useful source of information for these future plans.
Figure 2 The current structure of the service at the site suggests that initially large vertical services may be necessary for the initial scale ups. The use of lower cadre of clinical staff beside doctors may be suitable cost effective and safe. The necessity of good monitoring and evaluation systems, good counseling services to avoid erosion of already existing strategies and increased high risk behaviour particular in the first month post circumcision. The technique appears not to be a critical matter, though a single method that is simple and safe for each site would be wise. Models such as the national Blood Transfusion services which are vertical, with strong central administration and satellite linkages may prove most effective. The costs benefit suggests that this may be an attractive strategy to many of the low income countries where HIV infection has had the greatest impact. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06037f1.jpg] |
| |||||||||

{kind=link}