 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
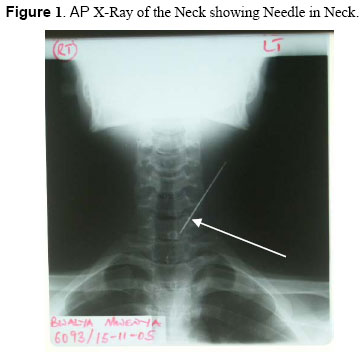
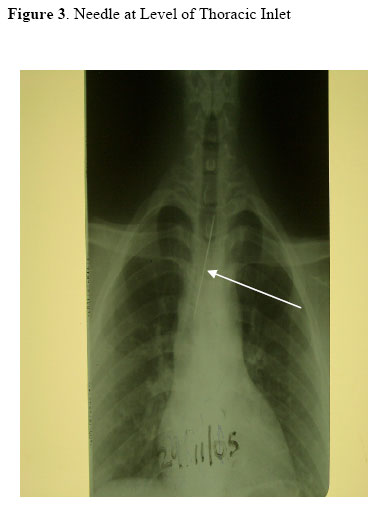
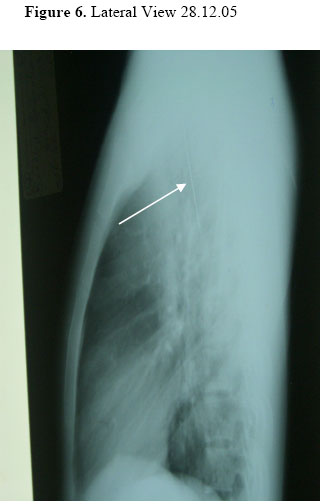
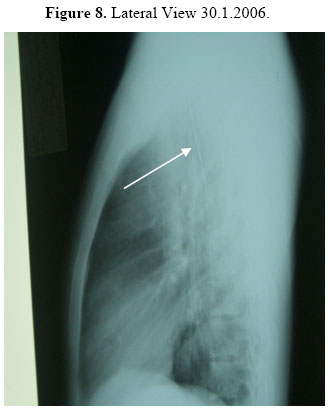
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 105-108 Needle in the Chest: A Case Presentation D.D. Mugala1, D. Datta2, E.P. Musonda3, Chomba Sikasote4 1Consultant Surgeon, Nchanga South Hospital, 2Anaesthetist, Nchanga South Hospital, 3Consultant Anaesthetist, Konkola Copper Mines Hospitals. Zambia, 4Consultant Surgeon Konkola Mine Hospital Correspondence to: Dr. Duncan D Mugala, Nchanga south hospital, P/B KCM 2000© Chingola Zambia. E-Mail Duncan.Mugala@kcm.co.zm Mobile +26096999957 Code Number: js06040 The occurrence of foreign bodies in the chests of adults is rare and when it does occur it is usually as a result of trauma. We present a case of a sewing needle in the chest of a healthy young man. The needle pricked him in the left posterior triangle of the neck and migrated and lodged in the superior and posterior mediastinum. This was successfully removed. Introduction The radiologic and clinical findings of foreign bodies in the chests of children are well recognized but foreign bodies in the chests of adults are rarely seen and the radiologic findings of these unusual circumstances have rarely been described. Tae Jung Kim1 et al has classified various thoracic foreign bodies into three types according to their cause: Type I, Aspiration, Type II, Trauma or Accident; Type III, Iatrogenic. In children foreign bodies in the chest are usually due to aspiration. The causes of foreign bodies in adults are more frequently iatrogenic or traumatic although aspiration has been implicated in some adults with some CNS dysfunction Case Presentation We present a case of a sewing needle in the chest of a healthy young man. A sewing needle pricked a 22 years old young man on the evening of 28th October 2005, as he was about to sleep. The needle had been left on the pillow and as he reclined the needle went in on the left side of his neck in the posterior triangle. The family members tried to pull the needle out using the cotton thread, which was still hanging outside the neck but the thread broke and the needle slid even deeper. He was taken to the local clinic and some how after a delay of over two weeks, he was admitted to the District Hospital where X-rays were done and the needle was identified as being in the neck on the left side (Figure 1). Ten days later he was referred to a tertiary hospital where further X-rays were done. At this stage the needle was seen to have migrated across the midline towards the right. He was kept in the hospital for one week and discharged on 1st December 2005, for some unspecified reasons the needle was not removed. He stayed at home for two months going from hospital to hospital until he finally came to our hospital for the surgery to remove the needle from his chest. Fortunately the local Lions Club heard of his plight and came to his aid and paid for his operation. Radiographs done on the 30th of January 2006 revealed that the needle had move from left to right and was lodging in the superior and posterior mediastinum (Figure 4). Preoperative evaluation We found a young adult male in good general condition. He had no fever, dyspnea, or pallor. He was not cyanosed or jaundiced. There was no pedal oedema. His Blood Pressure was 116/73mmHg and his Pulse was 82/minute. The apex beat was not displaced. There were no murmurs. The abdomen was normal Respiratory System showed a central Mediastinum with no subcutaneous emphysema and normal resonance on percussion. Air entry was equal in both lungs. There were no adventitious chest sounds. The ASA Grading was Grade 1. His airway was assessed as A1. Investigations done His haemoglobin was 12.8g/dL. Grouping and X-Match ordered and new X-Rays done. A Right Thoracotomy was performed on 31st January 2006. The 5cm long needle was found lying in front of the Oesophagus and behind the Trachea and the right main bronchus (see X-ray 5). The tip was pointing downwards and to the right, it was beyond the Vertebra and just about touching a big venous channel (Azygos Vein). To remove it, the needle was eased anteriorly away from the venous channel and pulled into the pleural cavity and taken out. Postoperative period. The patient did well. All the vital parameters were well maintained; he was put on prophylactic Gentamycin and Ampicillin. The intercostals tube was removed after forty-eight hours and he was discharged from the ward on the fifth day. When reviewed two weeks, the patient was and was found to be doing well. Discussion occurrence and when adults present with foreign bodies, a few are due to aspiration following for example a difficult intubation, but by far the etiology is often either trauma1 or following a Foreign bodies in the chest in adults are not a common procedure like pace maker insertion, the Temporary pacing wires are often left behind, assumed not to cause problems. Sometimes however they may cause foreign body reactions and present as anterior mediastinal foreign bodies2. Some foreign bodies may erode from the nearby structures and migrate into chest commonly from the Oesophagus3, particularly fish bones10, and these will often present as posterior mediastinal foreign bodies. Some of these may present as abscesses 4 or bronchitis7 Our patient was a case of transcutaneous traumatic entry of the needle into the left side of the neck in the posterior triangle, the needle seems to have slid down over a period of three months to lodge in the superior and posterior mediastinum on the right side, somehow missing all the vital organs5, 10 found in this space namely; the ascending Aorta, the Trachea, the Bronchi, the Oesophagus, the Thoracic duct the Azygos vein and the Sympathetic trunks. The explanation to this can be that the needle followed the loose areola tissue in its course. The retrieval of such objects can often be achieved by mediastinoscopy. Unfortunately such procedures are usually found in highly specialized centers6 and the alternative is the performance of a Thoracotomy and removal of the foreign body under direct vision. The needle was retrieved successfully and the patient did well after the operation. The sewing needle is a common tool found in most homes. If left carelessly it can cause injuries. In this situation it entered the chest and needed a major operation to remove it. Health education on proper storage of these useful tools in the home must be emphasized whenever possible to avoid such injuries. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06040f3.jpg] [js06040f8.jpg] [js06040f5.jpg] [js06040f2.jpg] [js06040f1.jpg] [js06040f4.jpg] [js06040f7.jpg] [js06040f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}