 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
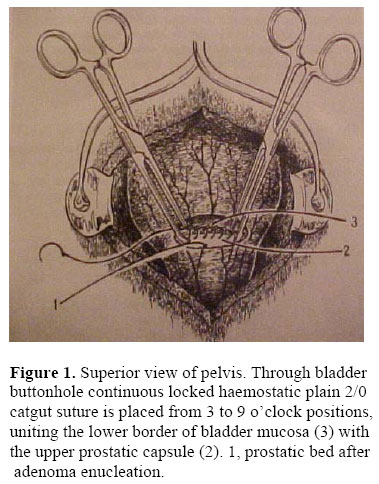
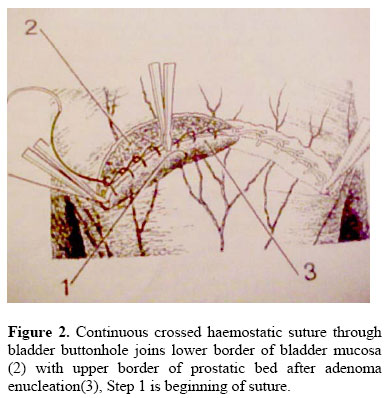
East and Central African Journal of Surgery, Vol. 11, No. 2, December, 2006, pp. 109-113 Feasibility of Open Simple Prostatectomy with Early Vascular Control Mohammed A. Labib, M.D, FRCS (Edin) University of Zambia School of Medicine, Lusaka, Zambia Fax: + 260 1 250753. Email: labib@zamtel.zm Code Number: js06041 Background: To describe open simple prostatectomy performed by applying lateral capsular transfixing sutures after adenoma enucleation and minimum operative haemorrhage. Introduction The state of urology in the developing world and certain tropical areas differs from that in the developed world in the incidence of certain conditions, prevalence of diseases unique to the region, availability of urological care and associated medical and social factors1. Communicable diseases such as sexually transmitted infections and genitourinary tuberculosis (TB) are very common. These infections are frequently inadequately treated due to poor patient compliance coupled with poverty and poor access to health facilities. Inadequate primary care leads to late presentation and high incidence of complications. With the burden of urological disease (Schistosomiasis, prostatic disease, urethral strictures, complex congenital abnormalities, vesico-vaginal fistulae, etc) overwhelming the region’s health systems, the provision of urological care in sub-Saharan Africa is less than adequate. This pessimistic view of urology in this part of the world is due to chronic under funding. There is a lack of trained urologists and endoscopic equipment is often absent or poorly maintained2. Medical treatment is unavailable for use in treatment of Benign Prostatic Hyperplasia (BPH). In Zambia, the University Teaching Hospital is the only tertiary health care centre in this country with a population of 9.9 million people3. Like many other cities in the developing world, Lusaka is one of the most urbanized in Sub-Saharan Africa. It has a population of 1.4 million in 2000 and a growth rate of 3.4%. The country’s only urology service, consisting of four urologists working as two units, provides urological care to the inhabitants of the Lusaka metropolis and also to patients referred by general surgeons from other parts of the country. Though communicable diseases are more common, 33% of the workload at UTH comprises BPH4. Other conditions include urethral stricture disease 17%, vesico-vaginal fistulae 11 percent, prostate cancer 8%, bladder cancer 7%, urolithiasis 6%, and complex congenital abnormalities 8% and miscellaneous other conditions 10%. Surgical treatment of BPH at the UTH in Lusaka is by transurethral resection of the prostate (TURP) and open prostatectomy. This care is provided against a background of shortages and chronic under funding which at worst prevents the purchase of the most basic health facilities such as intravenous fluids, antibiotics, surgical sutures and peri-operative basic ancillary investigations. Prostatic adenomectomy has not been performed in the developed countries a century ago, while it is still the main treatment in the developing countries as in Africa. The vesico-capsular approach is an extra capsular approach that provides anatomical exposure of the prostate because the incision is only 5 cm. above that of retro pubic approach. The lateral walls have the major veins and arterial pedicles called prostatic hila. It is found that applying lateral transfixing sutures at the level of the prostatic hila are useful means of controlling haemorrhage in prostatic adenomectomy. Methods Between April 1996 and December 2004, four hundred and twenty five (425) patients presented to the urology clinic at the University Teaching Hospital, Lusaka with symptomatic BPH. The followings are done for each patient: history taking, clinical examination including digital rectal examination, haemoglobin, haematocrit value, blood urea nitrogen (BUN), creatinine and abdominal ultrasonography. All the patients had given informed consent to undergo surgery. The inclusion criteria were symptomatic BPH, haemoglobin more than 10 gm/dl, creatinine less than 1.5 mg/dl, haematocrit more than 30%. Under spinal anaesthesia, a supra pubic incision was made exploring the urinary bladder and space of Retzius extra peritoneally; a 5 cm. incision was made between the inferior part of the bladder and the superior edge of the adenoma. Digital enucleation of the adenoma was performed. Sutures were placed at the posterior bladder neck and superior edge of prostatic capsule (Figure 1). Allis clamp was holding the posterior edge of the bladder neck. The initial transfixing suture was placed at the 3 o’clock position with simple 2/0 catgut. We continued to place simple crossed sutures to unite the inferior border of the posterior bladder neck with the superior and posterior borders of the prostatic capsule until arriving at the 9 o’clock position, where the suture was knotted (Figure. 2). A 3-way Foley catheter size 22 was inserted in the bladder and filling of the balloon with 30 ml. Saline to keep the catheter in the bladder neck and to avoid the dislodging of the balloon in the urethra. The bladder was closed and retro-pubic drain was inserted in the space of Retzius. To determine intra-operative and post-operative haemorrhage we measured haematocrit and haemoglobin 12 hours after the surgery. We also measured the amount of blood in the suction bottle. The duration of visible post-operative haemorrhage was monitored via the Foley catheter. Four variables and indicators we used for assessing the effectiveness of the haemostatic technique were as follows:
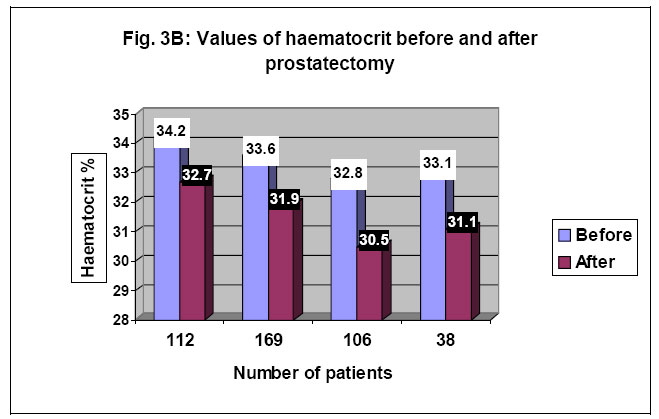
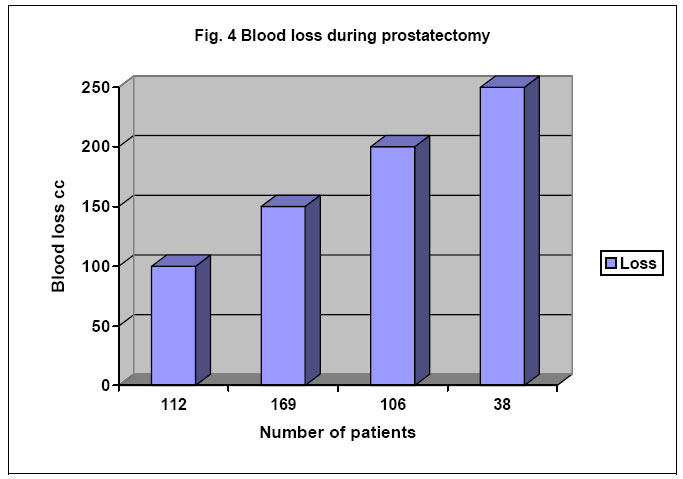
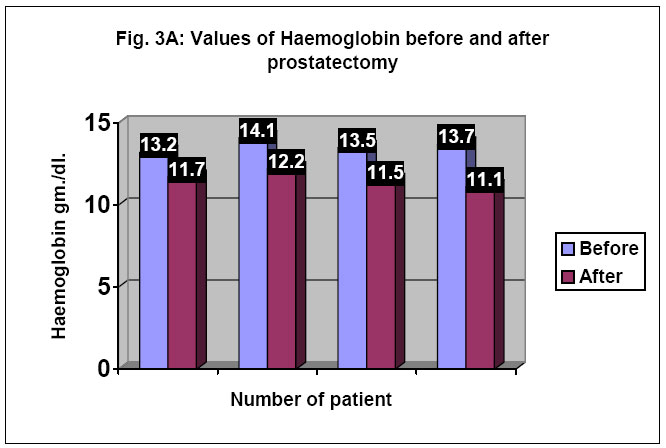
Results There was no intra-operative death. There was no blood transfusion for any of the 425 patients. Average pre-operative and post-operative operative haematocrit was 36.3% and 33.9% respectively. The median decrease was 2.7% respectively (fig. 3B). Figure 4 shows intra-operative blood loss measured by suction. The average blood loss was 125 cc., haemoglobin was 13.7 and 12.3 gm/dl respectively (fig3A). The median decrease was 1.85 gm/dl. respectively. Average pre-operative and post Discussion Benign enlarged prostate is an extremely common pathological condition in Zambia. A major problem in this condition is heavy intra-operative and postoperative haemorrhage. The Millin’s technique is an open procedure involving the intra-capsular approach4. Transfixing sutures are placed before the adenoma enucleation. There is a horizontal incision among several transfixing sutures placed where the vessels come from the dorsal penile vessels. This incision is 5 cm. below the vesico-capsular approach that we propose. Transurethral resection of the prostatic adenoma is the most common method. In less skillful hands or in cases of large adenomas it is associated with several complications, including severe bleeding which may require blood transfusion, perforation of the bladder, partial resection of the adenoma, and injury of the external sphincer5. The vesical capsular extracapsular technique that we propose is characterized by placement of transfixing sutures after adenoma enucleation. Because of extra capsular approach, there is no injury to the heavily vascularized prostatic capsule, which should explain the minor intra-operative and post-operative bleeding. It is reflected by the average post-operative decrease of only 2 gm. haemoglobin and 3% haematocrit. These informations indicate that the proposed technique is associated with a minimum degree of blood loss during surgery6. We do not pack the prostatic fossa. Retro-pubic drain is removed after 48 hours and Foley catheter after 5 days. Conclusion The haemostatic technique with extra capsular prostatic adenomectomy results in less bleeding. This technique is very suitable in our set up in Africa where there is no availability of endoscpic equipments and there are no experienced urologists. This technique can also be taught to the post-graduate students. There are no blood transfusion avoiding the hazards of blood transfusion like HIV disease and hepatitis. References
© 2006 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js06041f2.jpg] [js06041f1.jpg] [js06041f3b.jpg] [js06041f3a.jpg] [js06041f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}