 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
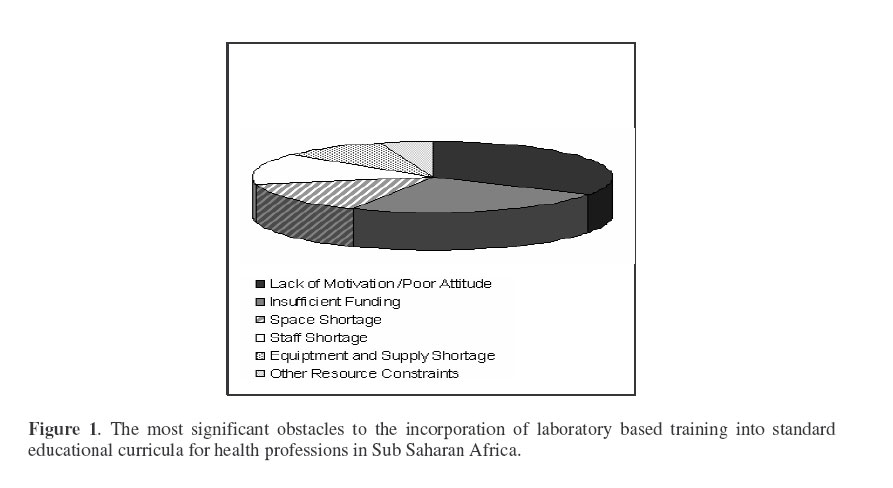
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 4-6 The Case for Surgical Skills Centres in Sub Saharan Africa: The Benefits and the Challenges. Dorman1, K.; Satterthwaite2, L.; Byrne3, N.; Debrew4, M.& Dubrowski2,3,5, A. 1Faculty of Science, University of Waterloo, 2The Surgical Skills Centre at Mt. Sinai, University of Toronto, 3The Wilson Centre, University of Toronto, 4Department of Surgery, Addis Ababa University, 5Department of Surgery, University of Toronto. Code Number: js07001 The purpose of this paper is to describe the educational and practice utilities of establishing Surgical Skills Centres. The paper also defines significant obstacles to the establishment of such centres in Sub-Saharan Africa.In 1996, the Royal College of Physicians and Surgeons Canada responded to the evolving roles and obligations of medical specialists by implementing a framework of core competencies called the “CanMEDS Roles” which define surgeons as medical experts, communicators, collaborators, managers, health advocates, scholars and professionals. A key competency expected of the medical expert is the demonstration of proficiency in procedural skills2. Europe and North America.Traditionally, procedural skills have been acquired through residency training programs, which incorporated graded-responsibility in the operating room3. However, the introduction of new technologies, ethical considerations regarding practice on patients and high-stress environments, minimize learning and limit standardization of practice3 and make patient-based training less than an ideal venue for the acquisition of primary technical skills4. Technical skills training laboratories may address some of these issues. They aim to provide instruction in fundamental procedural and technical skills, thus building resident confidence, creating a safer environment and facilitating productive time usage. The Surgical Skills Centre (SSC), Canada’s first skills training laboratory, was established in 1998 by the University of Toronto to provide opportunities for surgical skill acquisition outside the operating room. Educational principles of skill repetition and feedback guide the delivery of the numerous training programs provided by the SSC to undergraduate medical students and postgraduate trainees from all divisions of surgery and hospital affiliated groups. The primary focus of the Centre is, however, the Core Curriculum course for first-year surgical residents, consisting of 26 time-protected, 2-hour hands-on sessions. These sessions are proctored by expert surgical faculty members. The success of these sessions depends mainly on the development of a cadre of such experts who can prepare and deliver the Core Curriculum course. Africa.The Sub-Saharan African continent presents a new set of challenges for medical educators. With rapidly rising populations, increasing maternal and infant mortality rates, and the growing number of HIV/AIDS cases, Sub-Saharan African countries are experiencing critical shortages of health personnel in surgery, obstetrics, midwifery, and nursing. In Ethiopia, the density of physicians per 1000 people is 0.037 with even lower ratios in surgery where a skilled service provider attends to only 8% of pregnant women6. The effect of these shortages is an increase in practice loads to cope with patient volume. The result of heavy practice loads is a diminution of attention to the practitioners’ educational responsibilities. Low salaries, fear of contracting HIV/AIDS, and lack of support for innovation in education have added to the difficulties in the recruitment and retention of health care personnel. One way to circumvent the recruitment and retention problem is through the creation of skills training laboratories capable of enhancing procedural techniques by enabling competent clinical faculty, nurses, and midwives to train a multitude of trainees. Unfortunately, history shows that many developing countries’ initiatives fail mainly because of the lack of sustainability8. The technology and infrastructure have been developed and implemented; but the promotion of necessary support structures, such as trained indigenous human resources, is often neglected. The implementation of new health profession educational technology may thus prove costly and Unfortunately, history shows that many developing countries’ initiatives fail mainly because of the lack of sustainability8 . The technology and infrastructure have been developed and implemented; but the promotion of necessary support structures, such as trained indigenous human resources, is often neglected. The implementation of new health profession educational technology may thus prove costly and ineffective unless there is careful prior consideration of strategies necessary for sustainability. Laboratory based skills training is expensive in terms of faculty time and commitment since at least one expert heath professional must be present to train every four junior trainees8. Current low clinician to patient ratios does not permit the luxury of an expert stepping out of a clinical setting to teach. Therefore, to achieve educational sustainability, cohorts of highly motivated medical educators and clinicians must first be trained. A common institutional interest and motivation in “training the trainers” must be advanced as a priority for all African medical schools. With the interest and commitment of Sub-Saharan African health care system decision makers, the initial steps towards developing laboratory driven training can be initiated. Informal assessment of motivationIn May 2006, as part of the Bethune Round Table, the University of Toronto Surgical Skills Centre hosted a workshop dedicated to “Surgical Education for Africa”, led by Dr. Milliard Derbew (Addis Ababa University, and Fellow, Office of International Surgery). Ten surgeons from developing countries participated. The workshop concluded with the question “What are the most significant obstacles that prevent the creation and implementation of a surgical skills lab in your country?” The three themes that emerged were:
Responses regarding motivation and poor attitude, which emerged as the largest obstacles, included several sub-themes:
Workshop participants viewed the institutionalization of education of health professionals as a crucial component in the improvement and sustainability of the current health professional numbers. Specifically, the acceptance of training new cohorts of trainers in basic and specialized clinical skills will become a priority of the participating medical schools. However, for these changes to occur, both top-down and bottom-up motivational changes within the health profession education system must first take place. Acknowledgements The authors would like to thank Dr. Massey Beveridge and Dr. Andrew Howard (Office of International Surgery, University of Toronto) for workshop support. We also wish to thank Dr. Helen MacRae (D. H. Gales Director) and the University of Toronto Surgical Skills Centre staff for organizing and hosting the workshop. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07001f1.jpg] |
| |||||||||

{kind=link}