 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
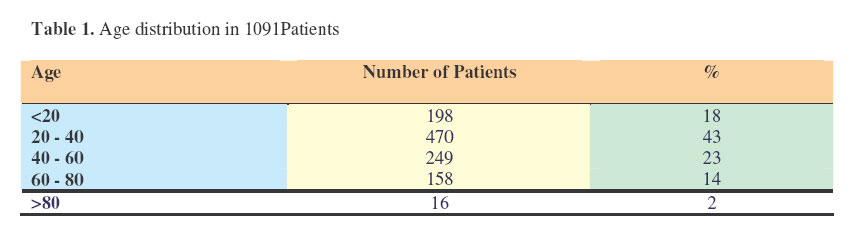
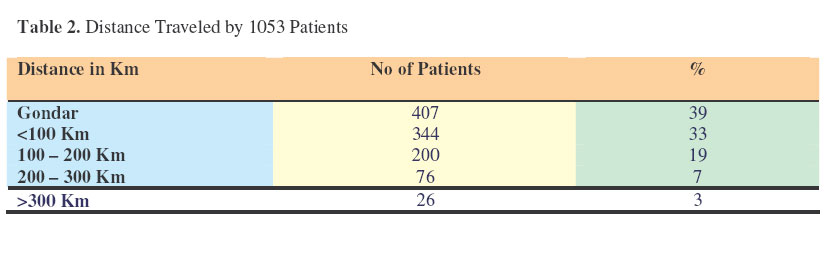
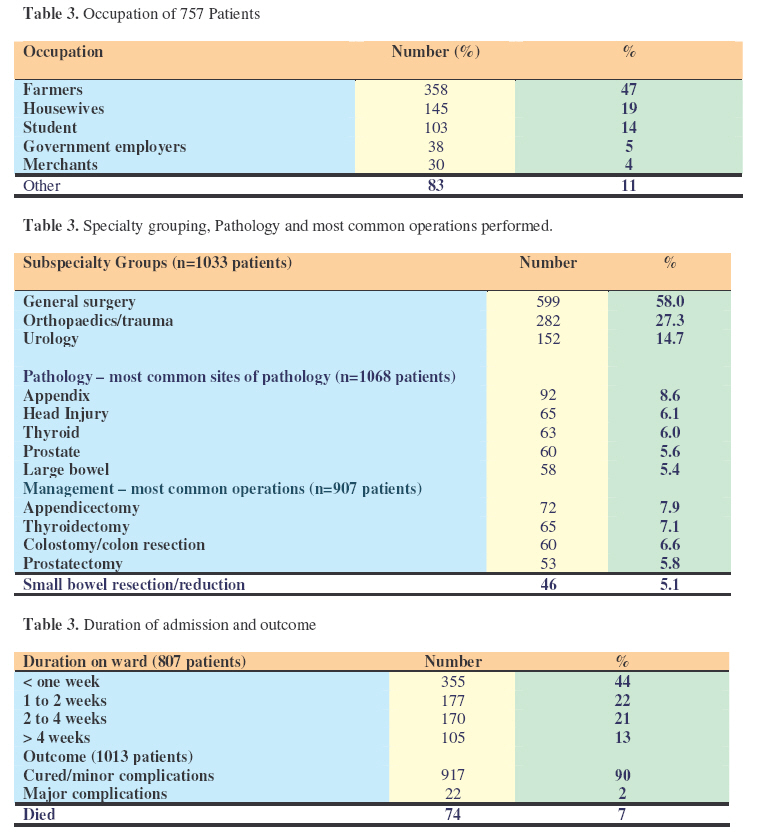
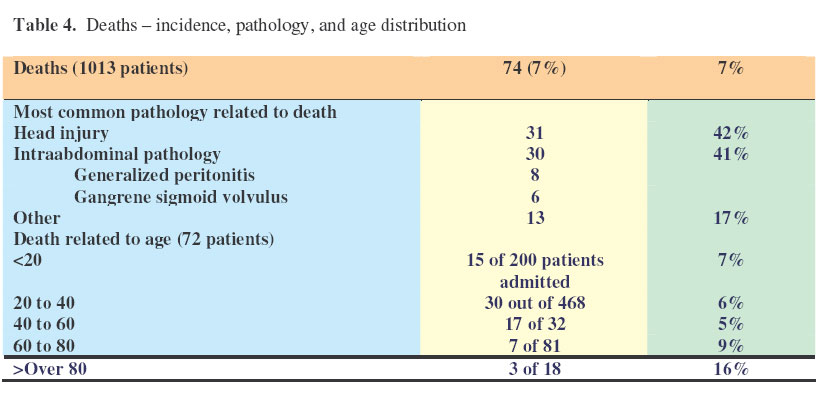
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 12-18 One Year Audit of Surgical Admissions at Gondar University Medical College Mensur1,Y.; Gebretsadik2, B.; Gashaw3, M. & Johnstone4 , J. M. S. FRCS (E), 1Dean, Gondar University Medical College, Gondar, Ethiopia,2Lecturer, Department of Surgery, Gondar University Medical College, Gondar, Ethiopia, 3Consultant Surgeon, Department of Surgery, Gondar University Medical College, Ethiopia, 4Leicester Gondar Link, Department of Child Health, Leicester Royal Infirmary, Leicester LE1 5WW Code Number: js07003 Background: The new University of Gondar enrolled surgeons for post graduate training in November 2003. A new surgical curriculum was designed in partnership with the Leicester Gondar Link. Admissions to the Department of Surgery over twelve months were subject to audit. The objectives of the audit study were to introduce a new concept, to review the surgical experience of the Department, to support organizational change, to integrate audit into post graduate training, and to measure and improve the quality of the service. Introduction Audit –carrot or stick – loved or loathed - is as critical to surgical experience as the knife is to skin. It provides raw data of need, is merciless in its objectivity, drives standards, and discloses challenges for receptive mind. In the United Kingdom, the value of audit was recognized at both governmental and professional levels, as part of National Health Service Reforms in 19891 and by the Royal College of Surgeons of London in the same year2 . Gondar is the second city of Ethiopia and the capital of the Amhara Region. The new University of Gondar enrolled its first students in 2004, as part of an overall expansion of education and health services in Ethiopia. As part of the reorganization, the previously named Gondar College of Medical Sciences (GUMC) has been renamed the Gondar University Medical College.In keeping with its new status, the College was instructed to introduce postgraduate surgical training. The Leicester Gondar Link is an affiliation of health care workers in each city. Amongst other activities, the Link has supported the GUMC in the introduction of postgraduate surgical training. In 2003, a four week period of surgical admissions was subject to audit in an attempt to gauge the experience of the surgical department. The practicality and the helpful results of the provisional study encouraged a move forward to a more detailed audit over twelve months. This paper describes the introduction of audit to the Surgical Department of the GUMC. The term audit is used in its literal and broad sense – an examination of accounts by authorized persons. The broad objectives of the present study were to introduce the concept of audit, record a profile of surgical practice, reinforce the need for organizational changes, incorporate audit into the postgraduate training programme, and to consider issues of quality. Material and MethodsData was collected on overnight stay patients admitted to the surgical department of GUMC over a twelve month period from 1st October 2003 to 30th September 2004. Day care patients were excluded. The information collected was wide and included personal details of name, age, sex and address; medical details of diagnosis, immunological and nutritional status, surgical management, postoperative complications, and outcome; and administrative detail of identification, date of admission, and duration of stay. The audit format was adopted from that used by the surgical unit of the Leicester Royal Infirmary3, modified for local conditions. Admission details were recorded by junior staff on a duplicated summary sheet on the day of discharge. One copy of the summary sheet remained in the clinical notes and a second was returned to the audit office. Details were then coded by a junior surgeon supervised by a named consultant, using a descriptive six letter code for diagnosis, operative procedure and complications. Results A total of 2500 operations were recorded, during the period of the study. From these records, 1900 inpatients admitted for a minimum of one night were eligible for the audit study. Of those eligible, adequate clinical detail was available for 1096 (58%) patients to be included in the study. In some patients, clinical detail was adequate but incomplete, and tables have been adjusted accordingly. For each item of data, the numbers of patients included are listed in brackets. The distribution of age, sex, and occupation of patients, and the distances traveled by patients from home to hospital are listed in Table 1. By age, 18% of patients were under 20 years, 43% were between 20 and 40 years and 16% were over 60 years. Table 2 shows the distance traveled to Gondar in 1053 cases. A total of 39% of patients were from Gondar while 33% lived outside the city but within a 100Km radius. Of the 1096 patients whose sex was recorded, 749 (68%) were males and 347 (32%) were females. Patients’ occupations were recorded in only 757 cases; 47% were farmers, 19% housewives, 14% students, 5% government employees, 4% merchants and 11% others (Table 3). Subspecialty grouping, common site of pathology and most frequently performed procedures are listed (Table 4). Patients were broadly distributed into three subspecialty groups, ‘General Surgery’ 58%, Orthopaedics and Trauma 27%, and Urology 15%. The five most common sites of surgical pathology among 1068 patients were appendix (9%), head injury (6%), thyroid (6%), prostate (6%), and large bowel (5%). Correspondingly, the five most common procedures among 907 operations were appendicectomy (8%), thyroid resection (7%), colonic resection and or colostomy (7%), prostatectomy (6%), and small bowel resection and or reduction (5%) Duration of stay for 807 patients and outcome for 1013 patients, defined as cured/minor complication, major complication and death, are listed (table 3). A total of 44% of patients remained in hospital less than one week, 22% between one and two weeks, 21% between two and three weeks, and 13% over three weeks. The outcome for 88% of patients was cure or improvement, for 5% complicated, and 7% died. Deaths among 1013 patients, the associated pathology and age distribution were as shown in Table 4. Seventy four patients died in hospital; 31(42%) of them died as a result of head injury, and 30 (41%) of intraabdominal bowel pathology. DiscussionA profile of experience and practice of the surgical department of the GUMC is well illustrated by this audit. Differences between this and comparable studies in the United Kingdom are stark and challenging; notably the age distribution, the inaccessibility of surgical services to the majority of the population, and the weighting of trauma and infection in contrast tot drive such a project forward the must be malignancy and degenerative disease. The results emphasized5. serve as a reminder of the adjustments that must be made by those involved in comparable link projects. The objectives of the study were to introduce the concept of surgical audit; to quantify the surgical experience of unit; to consider change within the unit based the results of the study; to build audit into the postgraduate curriculum; and finally to consider issues of quality. In this, the objectives are wide ranging and extend beyond the more conventional concept of audit where the emphasis is on quality of care4 . Audit – a new concept The introduction of a new concept is challenging, nevermore so than audit. Surgeons the world-over are practical. They will strive for their patient and in pursuit of their skills, but begrudge administration. Arguably, this study gives a fair picture of surgical practice in Gondar. The data in this study is incomplete; details were adequate in 58% of possible 1096 patients. Nevertheless, 58% for a new project is a considerable achievement. Moreover, it is probable that extrapolation of the data gives the broader picture. As there was no recognizable pattern of the patients omitted from the study, it is possible to consider that those included are a random selection of the whole. On reflection, different reasons for the shortfall of data are evident. The database was too ambitious, complex, and wide ranging. In particular, details of immunization and nutritional status were confusing and lacked definition. Inevitably, there were gaps in the clinical notes; for example, surprisingly few postoperative complications were recorded. The original coding of pathology and operative procedures proved difficult to adapt to local surgical practice, and has since been substantially modified3 . Although data was collected at intervals, encoding and entry to a database was left to the end of the year. Difficulties could have been recognized and rectified early, if data had been entered at frequent intervals. Finally, motivation of staff to a new project cannot be assumed and the need for a named consultant to support junior staff and to drive such a project forward the must be emphasized5 . Surgical experience Only patients admitted to the adult wards for one night or longer were included in the study. Day care patients, outpatients undergoing minor procedures and those admitted to the children’s wards were excluded. The profile is therefore weighted towards adults with more severe pathology. The male to female distribution among patients was of 2: 1. The figure is curious; it is explained in part by the nature of surgical pathology. Trauma is more common in men; of those admitted with head injuries were 61 male and 6 female. Functional bowel disease is more common in men; of those admitted with large bowel volvulus, all 15 were male. Nevertheless, there is a perception that for social and cultural reasons, it is harder for women to gain access to hospital. Demographic details in the study clearly illustrate the rural community has problems with access to surgical care. 39% of patients in the study lived in Gondar, a city with a resident population of 180,000. This compares with only 61% from the rest of the North Gondar Region, a region with a population of over 4 million. The reasons are many; education, wealth, availability, and above all transport. The scarce transport available is costly and many roads, particularly in the rainy season, are impassable. The uneven distribution of admissions compared with distance traveled is discussed further below. The predominance of farmers, 47% of patients admitted, reflects the agrarian weighting of the population. The age profile, 43% of admissions amongst patients aged between 20 and 40 years, reflects in part the age profile of the population, and in part the balance of pathology with trauma and infection relatively common in contrast to degenerative disease and malignancy. Listing of the most common sites of pathology and the most common operations underlines the amount of major surgery undertaken by the unit. To the Western observer, the prevalence of thyroid disorder and function bowel obstruction of both large and small bowel is striking. Outcome after surgery appears optimistic; major complications were only reported in 2% of patients. Outcome was poorly defined and postoperative problems probably under reported. For example, there were no records of postoperative chest complications, deep vein thrombosis, or wound dehiscence, and postoperative sepsis was rarely mentioned. The overall stay in hospital was relatively long, more than half of the patients remained in hospital over seven days. Length of stay was often determined by social factors and faulty administration. Paradoxically, prolonged stay was often the result of an error in the admission date or delayed operation rather than postoperative complications. Although there was no routine screening for HIV, many patients showed clinical manifestations of AIDs. An attempt was made to record the immunological status of patients on clinical evidence but the results were unclear and comment would be unhelpful. Organizational changeThe results of the audit served to strengthen the argument for change within the department; reorganization of the team structure, sub specialization and increase in consultant numbers from five to eight. Patients could be broadly placed into three specialty groups; general surgery (58%), Orthopaedics/trauma (27%), and urology (15%). The apparent low figure of 27% for trauma/Orthopaedic is explained by the patient selection. The vast majority of fractures are treated on a day basis. Within each specialty group there were particular surgical challenges; for example, complex bowel and thyroid surgery, the management of osteomyelitis and complex fractures, and nephrolithotomy and urethral stricture. As the regional referral centre for the Amhara, there is no alternative but to accept such challenges. The distribution of specialty groups reinforced the direction of change. Previously, all consultants practiced across a wide spectrum. However, it is generally accepted that complex surgery is better concentrated in the hands of a limited number of surgeons, each surgeon having appropriate experience and training. To meet the challenge, the department has been subdivided into three units, each remaining ‘general’ but with a subspecialty interest in gastroenterology, Orthopaedics or urology. In addition, five Gondar consultants have visited surgical units in Leicester to enhance their experience of clinical method, management, teaching and research in areas of individual interest. Postgraduate curriculumThe value of audit in medical education is recognized6 and the discipline has been accepted as an integral part of the new postgraduate surgical curriculum. Trainees are responsible both for the printout of audit data and for organising monthly morbidity meeting. During the trainees’ third year, they will undertake a clinical research project based on audit outcome. Five useful projects have been considered. Two projects explore further service developments, that the thoracic and paediatric workload be evaluated with a view to justifying further areas of sub specialist interest. Two projects examine quality of care, the surgical management and outcome of intestinal obstruction and septic arthritis. A fifth project study concerns demographic problems referred to above and the provision of surgical services to rural areas. Data clearly indicates that the number surgical admissions are inversely related to the distance traveled (Table 1), although the population within the different distance bands is judged to be comparable. Although there is some peripheral spill to district hospitals in adjacent areas, the numbers are small and the level of care offered is very basic. It is a hard reality that a patient with an acute surgical problem living more than 100Km from Gondar has virtually no chance of reaching hospital. To explore the problem further, funds have been secured for each trainee to spend four weeks in one of three district hospitals during the third year of the rotation. Funds also provide for consultant support and supervision. QualityThe audit cycle provides a baseline of surgical practice, identifies a problem, an adjustment is made, and the outcome observed -closing the feed back loop7. The present audit takes us half way; within the limits of completeness of the study, a base line is provided and problems are evident. The first and most far reaching problem is the inadequacy of services to the rural population as discussed above. A second problem is the mortality rate among patients admitted with head injury. Data for patients with head injury is presented in Table 3. The data lists 67 patients of whom 61 were male, 21 suffered a depressed fracture, 4 underwent elevation of the depressed fracture, and the overall mortality was 46%. By any standards, the outcome can only be described as disappointing. While the outcome can partly be explained by severity of the injury, it also reflects lack of policy, lack of surgical skills and paucity of high dependency care. As a result of these figures, a policy is to be drafted and neurosurgical skills enhanced. A high dependency unit has recently been opened. It is hoped that the benefit will be apparent in future audit – thus completing the second half of the audit cycle. Early and late post operative morbidity, mortality and outcome reflect quality of care and are the essence of clinical audit. Furthermore, such data allows for comparison between different surgical centres. However, such comparison depends on accurate recording and clear definition of data and on long term outpatient follow up. In this study, data is limited to the period of admission; longer term follow-up of patients is clearly not possible given the social and demographic restrictions. Although the mortality rate of 7% is meaningless in terms of a national enquiry such as the National Confidential Enquiry into Post Operative Deaths8, the figure serves as a marker for Gondar on which further change can be monitored. SummaryAn audit of admissions to the surgical department of the GUMC over twelve months was undertaken. The purpose was to establish a rational basis on which to develop postgraduate training and to introduce the concept of objectivity. The data confirmed the surgical experience available for training purposes was more than adequate, reinforced the need for organizational change, and highlighted issues of quality. Organizational change has been made; consultant numbers have been increased and sub-specialization introduced. Quality issues are being address and will be subject to further audit; in particular, inadequacies of services to the rural community and the poor outcome after head injury. Audit has integrated into the training programme, providing data for morbidity and mortality meetings and clinical research. It is accepted that data was only adequate for 54% of patients. It is probable that morbidity and possible that mortality is under-reported. Nevertheless, it is argued that data can be extrapolated to show trends. The difficulty in introducing a fundamentally new concept must be appreciated and the need for constant encouragement by a lead consultant is emphasized. AcknowledgementFunding for this project was provided by the Vita Bailey Trust; secured through the Tropical Health and Education Trust 210 Euston Road, London, NW1 2BE, England to which we are grateful. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07003t3a.jpg] [js07003t5.jpg] [js07003t3.jpg] [js07003t2.jpg] [js07003t4.jpg] [js07003t1.jpg] [js07003t3b.jpg] [js07003t3c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}