 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
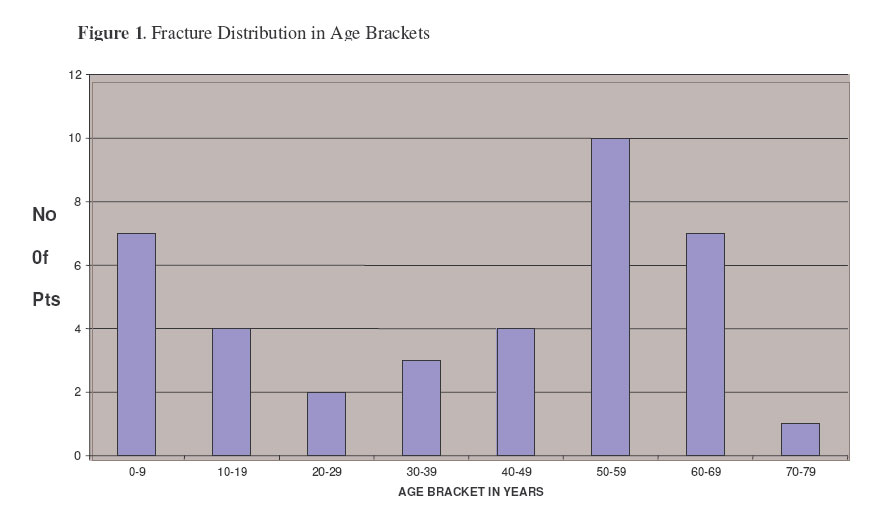
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 19-23 Non-Metabolic Causes Of Pathological Fractures in Kenyatta National Hospital in Kenya: A Descriptive Prospective Study. Oburu, E. & Ating’a, J.E.O. Corresponding to: Dr. Ezekiel Oburu, Department of Orthopaedics, KNH, Nairobi – Kenya. Email: oburue@yahoo.com Code Number: js07004 Background: Pathological fractures pose a major challenge to surgeon since he has to treat both the fracture and the pathology associated with it. This study was aimed at determining the pattern of non-metabolic causes of pathological fractures in Kenyatta National Hospital. Introduction The hallmark of a pathological fracture is one that occurs during normal activity or after minor trauma. By examining mummies, researchers have traced metastatic bone disease (one of the most common causes of pathological fractures) to as far back as 2400 years ago. Pre Colombian Incas and Egyptians of the third and fifth dynasties are reported to have had metastasis1 . Pathological fractures do indeed present a major challenge, as the surgeon has to treat both the fracture and the pathology associated with it. Management of these fractures will go along way to alleviate pain although it may not add days to the life of a patient; it will certainly improve the quality of the patient’s life. Review of our local literature reveals that no prospective study has been done on these fractures. Although Githae2 had carried out a study on pathologic fractures his was a retrospective study and it was done ten years ago prior to the intended study. Furthermore anecdotal evidence from working in the paediatric orthopaedic ward suggests that osteomyelitis contributes a significant percentage to these fractures but review of literature does not reveal documentation of this. The aim of this study was to determine the causes, site, presentation and management of these fractures. We also looked at the prevalence of the fracture among other fractures in the orthopaedic wards. Materials and Methods This was a prospective descriptive study over a period of 10 months, between April 2002 and January 2003. The study was carried out in the orthopaedic wards of Kenyatta National Hospital, which is a teaching, and referral hospital that also serves as a point of primary care for many people in Nairobi. All patients with a non-metabolic cause of a pathological fracture admitted to the orthopaedic wards were included in the study. Excluded from the study were patients refusing to consent to the study, patients with pathological fractures due to metabolic causes and patients from amenity wards. Permission to carry out the study was sought from the Ethical and Research Committee of Kenyatta National Hospital. All information obtained from the study was treated with utmost confidentiality and used only in the study. The wards were visited after admission and the fractures admitted were noted. The patients with pathological fractures were then reviewed. Upon consenting, the demographic data of the patient was taken. Data was collected by the use of a questionnaire designed for the study. A history was taken from the patient and a physical examination was carried out to try and establish the presentation, the site and the cause of the fracture. Investigations were carried out, both baseline, a full blood count, kidney function tests and specific investigation depending in the suspected cause. All patients were admitted with x-rays as it is the policy of the hospital to perform x-rays on all patients with fractures before admission. The data was entered and analyzed using Microsoft Excel version 2002 software. Proportions and means of relevant variables such as demographic characters, causes, sites, presentation and management of the fractures were derived and presented in tables, graphs and charts. ResultsA total of 38 patients were seen during the study period. The male: female ratio of 1:1. The total number of fractures in the group of patients was 53. The patients ranged in age from 1 to 74 years with a mean age of 40 years (standard deviation of 22.5); and a median age of 46 years. The age distribution is represented in the figure 1 below. During the months of April 2002 to January 2003 there were 2020 fractures admitted to the orthopaedic wards. Of these 53 were non metabolic pathological fractures. The average number of fractures admitted per day in the orthopaedic wards was 7.26. The prevalence rate of non metabolic pathological fractures among fractures admitted to the orthopaedic wards was 2.62%. There were 11 patients with primary malignancy, 10 with multiple myeloma (19 fractures) and one with osteogenic sarcoma. Table 1. The causes of pathological fractures.
Table 2. Causes of metastatic fractures
Of the 10 patients with osteomyelitis 7 were found in the first decade and 3 in the second decade with an age range of 1 to 16 years and a mean age of 8.5 years. There were 7 males and 3 females. Three other patients were classified as having benign causes of pathological fractures. One patient had giant cell tumour while another had polyostotic fibrous dysplasia. Unicameral bone cyst was the cause of fracture in the third patient. The fractures were distributed both in the axial skeleton and the appendicular skeleton. There were 24 fractures (45%) in the axial skeleton, of all these 23 fractures were in the spine and 1 fracture was in the fourth rib. There were 29 fractures (55%) in the appendicular skeleton with 25 (47%) in the lower limb and 4 fractures (8%) in the upper limb. It would be nice to see this diagrammatically Of the fractures that were in the spine, 7 were found in the thoracic region and 16 were found in the lumbar region. The patients with pathological spine fractures ranged in age from 35 to 65 years with a mean age of 55.1 years and a standard deviation of 9.9. The median age was 55.5 years. The ratio between fractures in the thoracic region to those in the lumbar region was 1:2.3. There were 9 patients with pathological fracture due to multiple myeloma, 3 due to carcinoma of the breast, 3 with carcinoma of the prostate, 1 had carcinoma of the thyroid and the cause was unknown in two patients. There were 22 patients with 25 fractures in the lower limb. One patient had a metastatic tumour in the fibula due to squamous cell carcinoma. There were 9 pathological fractures due to malignancy; 9 due to osteomyelitis, 5 had metastasis and 2 had benign bone disease. Of the 4 patients with fractures in the upper limb 2 had fractures in the humeral shaft due to multiple myeloma. One patient had a fracture due to osteomyelitis in the metaphysis of the humerus. The fourth patient had a fracture at the distal radius caused by a unicameral bone cyst. DiscussionThe majority of patients had pathological fractures due to malignancy which included those due to primary malignancy and metastatic fractures. Infection was the next common cause of fractures. There was a bimodal distribution of the fractures with children presenting early and the cause of the fracture as osteomyelitis and adults presenting late with malignancy. The first peak was in the first decade while the next was in the sixth and seventh decade. Malignancy due to metastatic disease and primary bone neoplasm formed a total of 76 % of fractures. This was expected as had been stated by Springfield and Brower3. That malignancy is the commonest cause of Pathological fractures. Githae2 in 1991 reported that there were 79 patients with 108 fractures. Our study shows that what may have been reported to be the annual incidence of pathological fractures due to metastatic disease in 1991 may have been under reported. The number of malignant pathological fractures in a period of 10 months was more than a third of all the fractures seen in Githae’s study of 10 years2. This is probably due to the fact that in a retrospective study one may not access all the data due to inadequate coding of the disease conditions associated with pathological fractures. Osteomyelitis was the only cause of pathological fractures in all paediatric patients seen during this study. Prior to the study, only anecdotal evidence had pointed out that osteomyelitis was a common cause of pathological fractures. In a prospective study of haematogenous osteomyelitis in children in Kenyatta National Hospital over a period of one year, Ngetich4 had about 7% of 73 patients who had a pathological fracture at the time of presentation. Despite the high percentage of paediatric patients with osteomyelitis as the aetiology of the fracture little in the literature has been written about pathological fracture due to osteomyelitis5. Access to health care is not readily available to all the patients who may have acute osteomyelitis in our set up and therefore a number of patients develop chronic osteomyelitis which may then lead to a pathological fracture. Wilson considers unicameral bone cyst as one of the most common causes of pathological fracture in children5, but in our set up it seems to be osteomyelitis. Also interesting to note, lung carcinoma was not one of the causes of pathological fractures. This concurs with Githae2 but differs from other authors. McLain and Weinstein6 found that Ca lung constituted 14% of all these patients the plausible explanation for this is that Ca Lung may not be one of the leading malignancies in Kenya as it is in other countries. There were more fractures in the appendicular (55%) skeleton than in the axial skeleton. The significant contribution of number of fractures due to osteomyelitis explains this. While fractures in the appendicular skeleton were caused by metastatic disease, primary malignancy and osteomyelitis, those of the spine were only due to metastatic disease and primary malignancy. Nonetheless most of the malignant fractures, 23 out 39, which is 59% of the fractures were in the spine. Sim7 notes that vertebral column is the most common site of skeletal metastasis. Most of the other malignant fractures were located in the lower limb. This is in keeping with what Rock8 states that a malignant pathological fracture is less likely to occur in the upper extremity than in the pelvis and lower extremity. Ninety percent of the pathological fractures due to osteomyelitis were located in the lower limbs with 60% being located in the femur. This finding is consistent with what was found by Ng’etich4 and Okoroma and Agbo9 in that bones of the lower extremities were more commonly involved, than those of the upper extremities. This may be related to the higher likelihood of trauma in the lower limbs which may precede the development of acute osteomyelitis10 and hence the development of chronic osteomyelitis which may finally culminate in the development of a pathological fracture. The lower limb is also weight bearing and hence with the stress it has to bear the incidence of pathological fractures is higher. The principal symptoms that patients with malignant spinal fractures presented with included back pain, inability or difficulty in walking, incontinence of stool and urine and paraesthesia. The most common complaint was inability or difficulty in walking, principally due to weakness of the lower limbs. Thirty six percent of the patients presented with both back pain and difficulty in walking due to weakness, with the weakness presenting after the back pain. Harrington11 explains that weakness of the extremities may not become apparent until months or years after the onset of back pain. It is observed therefore that a large percentage of patients in our set up present relatively late, months or years after the symptoms begun. Githae2 in his study noted that it could be that the patients presented early but it took some time to get to the referral hospital. Late presentation is also evidenced 21% of patients with malignant pathological fractures of the spine presenting with incontinence of urine and stool. Harrington11 states that loss of sphincter control is thought to be a late phenomenon and usually occurs only in patients with profound involvement. In this study, 45% of patients with lower limb fractures had a history of trivial trauma prior to the fracture. This was the most common complaint of pathological fractures in the lower limb. The hallmark of presentation of a pathological fracture is a fracture that occurs after mild trauma12 . These results compare with what Githae2 found that 32% patients with lower limb fractures presented with a history of trivial trauma Swelling as a symptom was exclusively found in patients with osteomyelitis. Swelling is one of the symptoms that patients with osteomyelitis present with as noted by some authors10. Ngetich4 found that pain and swelling were the most common modes of presentation with a percentage of 84% and 76% respectively. ConclusionThe most common cause of pathological fracture was bone malignancy with the peak age of patient in the sixth decade. The malignant causes of these fracture compares to what other authors have found. Osteomyelitis was the most common cause of pathological fractures in children. The sites of pathological fractures seen in descending order are the lower limb, the spine and the upper limbs. The major complaints in patients with spinal pathological fractures were back pain and difficulty in walking with a number of patients presenting late .Trivial trauma was the most common complaint in patients with appendicular skeleton fractures. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07004t2.jpg] [js07004f1.jpg] [js07004t1.jpg] |
| |||||||||

{kind=link}