 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
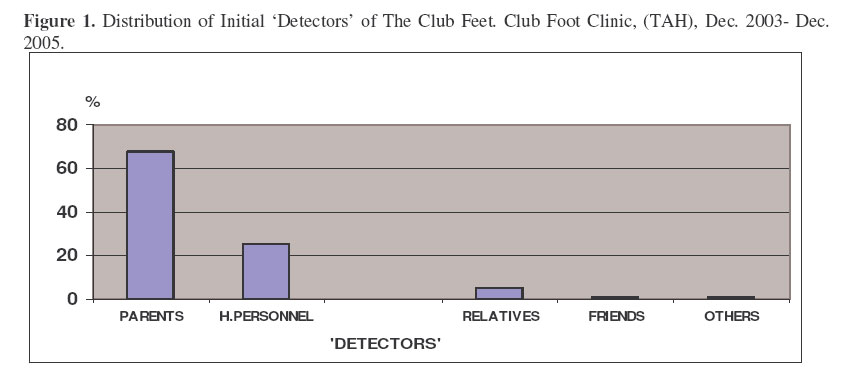
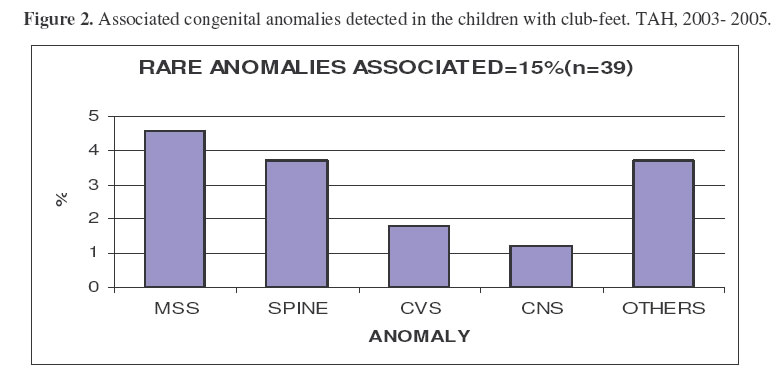
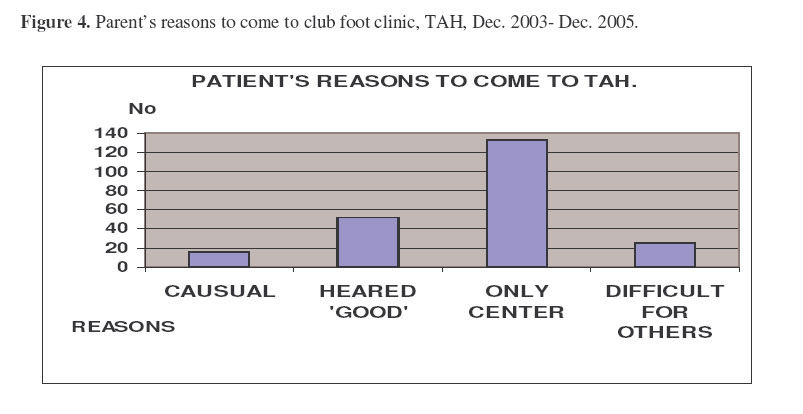
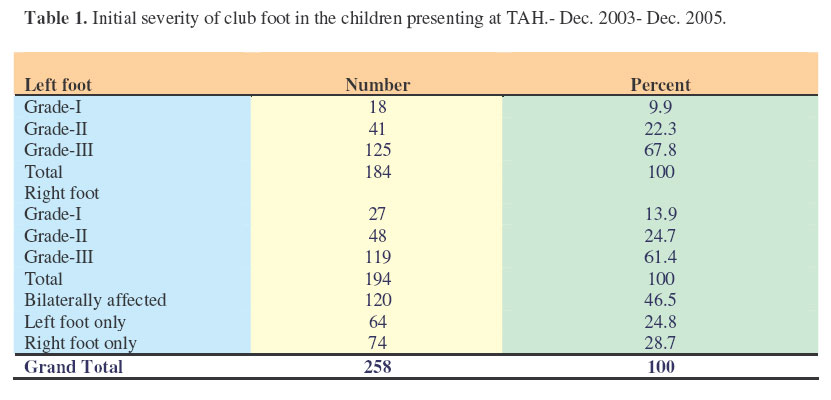
Management of Club-Foot at Tikur Anbessa Hospital; Addis Ababa, Ethiopia.Biruk, W.L. : M.D., FCS (ECSA), Asst. Prof. in Orthopaedic Surgery. Department of Orthopaedics, Addis Ababa University, Correspondance to: Dr. B. L Wamiso, P.O.Box: 122201, Addis Ababa, Email: lbiruklw@yahoo.com, Code Number: js07005 Background: “Club-foot”, congenital talipus equinovarus (CTEV) is a common congenital anomalies encountered in paediatric orthopaedics. This study was aimed at determining the pattern and the short term outcome of management of CTEV in Ethiopian children seen at our Club foot clinic at TAH in Ethiopia. Introduction Clubfoot or congenital talipes equinovarus (CTEV) has been recognized since the time of ancient Egyptians and well described by Hippocrates. Pleoarcheological case findings of bone dating over 2000B.C are available in museums even today1 . It is an important congenital anomaly of the lower limb & occurs in about 1-3/1000 live births on average. The main components of the deformity are: forefoot adduction, hind foot varus, inverted calcaneus under equinus talus, and medial displacement of navicular and cuboid bones. New molecularbiology studies confirmed that the deforming genes are active at the 2nd trimester; hence it is a developmental malformation. Incidence varies with Ethnicity and geography. (Reports of 0.5- 7/1000 do exist). The reported incidence in Black South Africans is 3.5/10002. Males are affected 2- 3 times and bilaterality occurs in half of the patients3. One nearly every four patients have a positive family history3,4 . The aetiology of clubfoot remains unknown. The three principal suggestions are: intrauterine moulding, neuromuscular imbalance and delayed intrauterine development 2,5,6,7,8. The later two are strongly advocated. Good classification is important to choose treatment modality and predict prognosis. The Pirani score developed by Dr. Shafique Pirani is currently widely used. It considers three signs on mid foot and hind foot, grading from 0-1 based on the severity. It also helps to decide when to do Tenotomy especially by less experienced health personnel. The Harrold-Walker scheme, based on the reducibility of the deformity by manipulation was widely used in the previous days3,9 . Deformity manipulability to neutral position is Grade-I (Mild), manipulability to within 20 degree from the neutral is Grade-II (Moderate), and Patients whose deformity (either varus or equines) could not be manipulated to with in 20 degree of the neutral are described as Grade-III (Severe)3 . Gentle manipulation and serial casting, Popularised by Kite in 1930, but well modified and scientific ground given by Dr. Ignacio Ponseti remains the best treatment of choice10,11 . Soft tissue release surgeries were begun in the late 1800s but now surgery is said a wrong approach to club-feet, with poor results and complications11 . It is also expensive for poor nations where higher club foot incidence is seen. Many studies have shown that club-feet treated with the conservative method (serial casting and manipulation) have been successfully corrected up to 90 %3,11. The success rate depends on initial severity, age at start of treatment, presence of neurological pathology, adherence to the standard protocols, family support and also experience in the correct manipulation and cast application. Any modifications of the standard treatment protocols due to economical reasons, poor compliance or lack of experience will lead to unpredictable poor outcomes11 . Laavege and Ponseti devised a functional rating system that has been widely adopted to evaluate outcomes of treatment. It incorporates such domains as patient satisfaction and pain, gait, heel position and range of motion6,7 . Club feet with poor short outcome outcomes definitely will end up with poor long term outcomes. Patients and MethodsUsing standardized pre-coded questionnaires, all the consecutive 258 (378 feet) patients with club feet (CTEV), aged less than two years, presenting to the clubfoot clinic in the study period from Dec.2003-Dec.2005 were interviewed. Taking prevalence of less than 4/1,000 live births, and working out the formula, n= (Z/E) 2 (P) (1-P) , the sample size was statistically more than adequate. Patients in different age categories were treated with different treatment protocols and the short term outcomes of these were compared. Operated patients were followed separately. The study was followed by the orthopaedic department. Statistical analysis was performed by EpiInfo-2002 software and SPSS/PC for windows version 11. For comparison of the dichotomous two proportions of outcomes, Chi-square and odds ratio were used to test statistical significance. ResultsA total of 258 children with 378 club-feet were studied. Three quarters (194/258) of the patients were males. The mean age at the initial presentation was seven months. Half of the children were first born and about equal number (142, 55%) were born in Health institutions. For those born in Health institutions, the mean birth weight was 2.8 Kg. In 182 (71%), the disease was noticed at birth. Most (77%) of the patients came from urban areas and 62% of the mothers were attending antenatal clinics of which 23 (9%) were told had high risk pregnancy. The mean maternal age was 27 years. Two hundred and twelve (82%) of the mothers were housewives. Half of the parents had a low monthly income of less than 25 dollars; 80 (31%) of the patients had free treatment. Prenatal ultrasound was done only for 86 (33%) of the mothers. CTEV was bilateral in120 (46.5%) of patients. There was positive family history in 31 (12%) children. In 71% of the children, the disease was noticed right at birth. In the majority the disease was severe and in 176 (68%), the problem was noticed by parents (Figure 1). In a quarter of the health institution born patients, the diagnosis was initially missed. Twenty six (10%) children were taken to bone setters. Thirty nine (15%) children had other associated congenital anomalies and motor milestones were delayed in 67 (26%) of the children (Figure 2). Half of the patients did not have their first cast for more than three weeks after they were referred to the club-foot clinic with 129 of the children spending more than a month before getting any treatment. About two thirds (157, 61%) of the patients said that the clubfoot clinic at TAH was the only centre they knew of (Figure 4). The severity at initial assessment was as follows (Table 1):
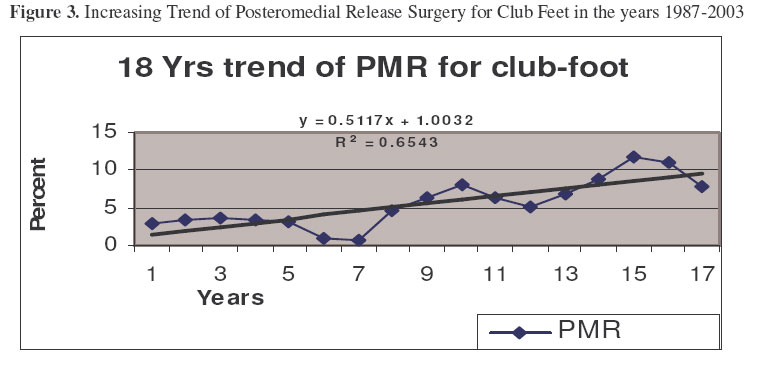
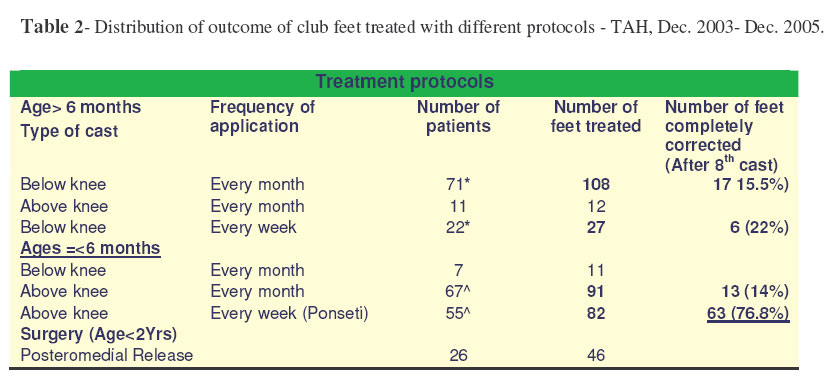
Fourteen (5.1%) of the patients had a significant sore from the cast. Only 60% of the patients requiring clubfoot shoes got them and this also took an average waiting period of 3-4 months. Maximum casting was 17 times but short term evaluations were done after the 8th cast. Only in 23 (9%) of the patients was the cast removed with-in an hour before the reapplication. Posteromedial release (PMR) was done in 46(12%) feet and 57% of them waited for more than three months for admission. In the last two decades there was an increasing trend of performing PMR, which has markedly started to drop in the last two years (Figure 3).In unilateral condition, there was 2.5 cm calf circumference difference post PMR, which is significantly higher from those treated with cast (1.1cm). After the 8th cast (unless complete correction has been achieved earlier), in the under 6 months group, 63 (76.8%) feet were completely corrected using the standard Ponseti method as compared to correction obtained only in 13 (14%) feet using Ponseti technique every month (Table 2). This was statistically significant with chi-square of 62 and odds ratio of 20 at 95% CI .In the older ages, there was no statistically significant difference between using a short leg cast every month or each week.The results were poor. DiscussionMy study has revealed some surprising findings: Half of the children were first born and about equal number (142, 55%) were born in Health institutions but in a quarter of the health institution born patients, the diagnosis was initially missed. This leads to start the treatment late, hence poor short and long term outcomes5,7,11 . Twenty six (10%) children were taken to bone setters again training bone setters may help in Africa. In the majority of them (182, 71%), the disease was noticed at birth as mainly the disease was severe and easy to detect. Most (77%) of the patients came from urban areas and 62% of the mothers were attending antenatal clinics of which 23 (9%) were told to have high risk pregnancy. Alas how many rural children are left at home with out medical attention? The mean maternal age was 27 years and 212 (82%) of the mothers were housewives. Half of the parents have monthly income less than 25 dollars and 80 (31%) of the patients were treated freely. This may be one economic reason for poor compliance in African parents11 . Prenatal ultrasound was done only for 86 (33%) of the mothers and it is my feeling that detecting club-feet by U/S is still a long way for Africa. The condition was bilateral in120 (46.5%) and there was positive family history in 31 (12%) children, which are consistent with similar studies. In 71% of the children, the disease was noticed right at birth and in the majority the disease was severe and most (176, 68%) of the problem was noticed by parents. This is an area where educating the public using radios and TV may help. Half of the patients did not have their first cast for more than three weeks after they were referred to the club-foot clinic and an equal number (129) of the children spent more than a month before getting any treatment. By any standard this is very late and more has to be done to improve this11 . About two thirds (157, 61%) of the patients said that the clubfoot clinic at TAH was the only centre they knew of and came from very far regions. Opening more centres in the country may solve this problem. Fourteen (5.1%) of the patients had a significant sore from the cast. It is not bad as the clinic is new in our Hospital. Only 60% of the patients requiring clubfoot shoes got them and this also took an average waiting period of 3-4 months. Maximum casting was 17 times but short term evaluations were done after the 8th cast. These figures are rather shocking and improvements are on the way from our Department. Only in 23 (9%) of the patients was the cast removed with-in an hour before the reapplication. Posteromedial release (PMR) was done in 46(12%) feet and 57% of them waited for more than three months for admission. In the last two decades there was an increasing trend of performing PMR, which has markedly started to drop in the last two years .This is mainly due to the approval of Ponseti method by the department and simultaneous study and follow up which is started at this time. In unilateral condition, there was 2.5 cm calf circumference difference post PMR, which is significantly higher from those treated with cast (1.1cm). After the 8th cast (unless complete correction has been achieved earlier), in ages less than 6 months group, 63 (76.8%%) feet were completely corrected using the standard Ponseti method as compared to correction obtained only in 13 (14%) feet using Ponseti technique every month. 76% success is a lower figure, as the method is just adopted and there were no adequate trainings during that time. Improvements and better outcomes in the next follow-up results will be expected and I am sure my colleagues will report this soon. ConclusionsClub foot is a commonest musculoskeletal congenital condition in our Hospital and can be effectively treated using appropriate conservative methods. The outcome is better the earlier it is started. Pre-natal screening, post-natal neonatal examination and educating the public will decrease the chance of missing the problem at an early age. Proper training to practice the Ponseti technique may increase its success rate. All modified methods from the standard Ponseti protocol have poor outcomes and should be abandoned. Availability of more club foot clinics and supply of the necessary medical equipment will lead to improved outcomes. AcknowledgementI thank all the staff at the mother department. I dedicate this paper to my 8 months old terrific daughter, HLDANA (of course she has no clubfoot!). Dr. Woods help was there, as usual. I thank him for reviewing the manuscript and his wife, Anita for always visiting our department. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07005f4.jpg] [js07005t1.jpg] [js07005f1.jpg] [js07005t2.jpg] [js07005f3.jpg] [js07005f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}