 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
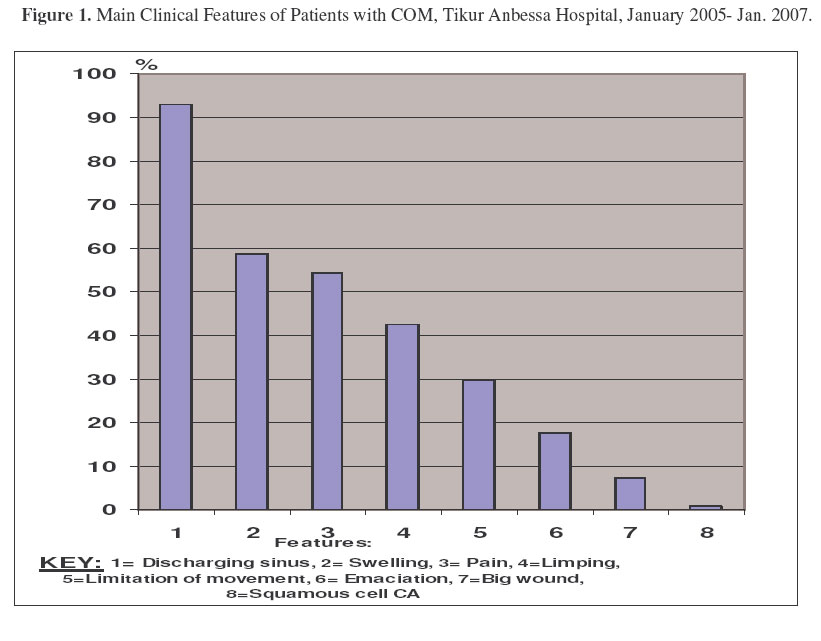
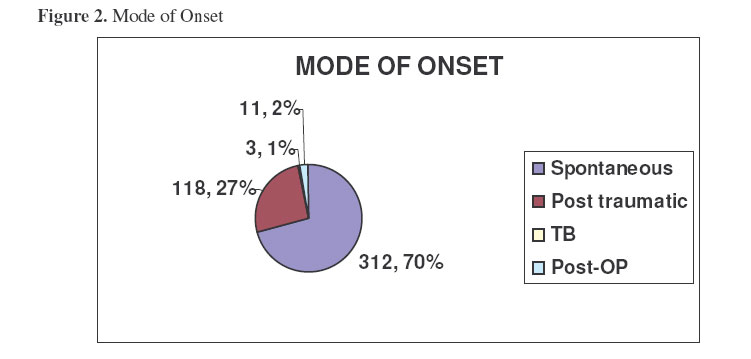
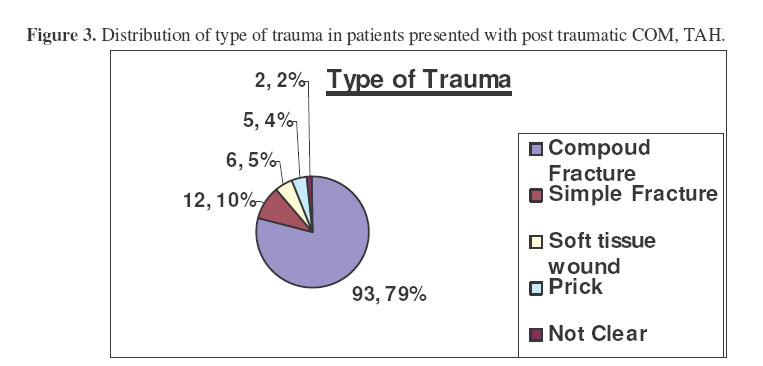
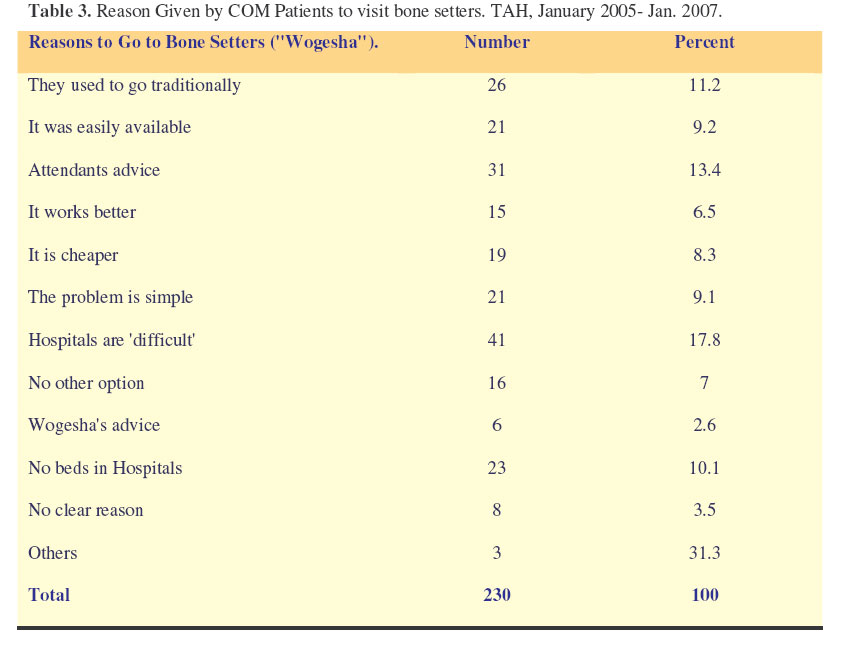
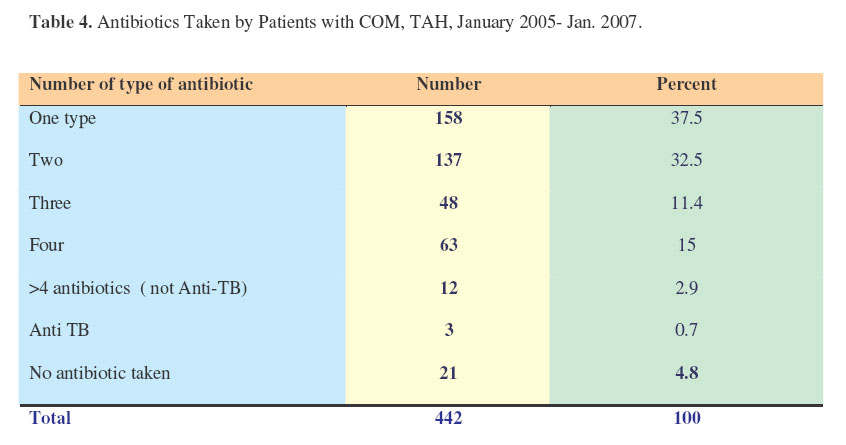
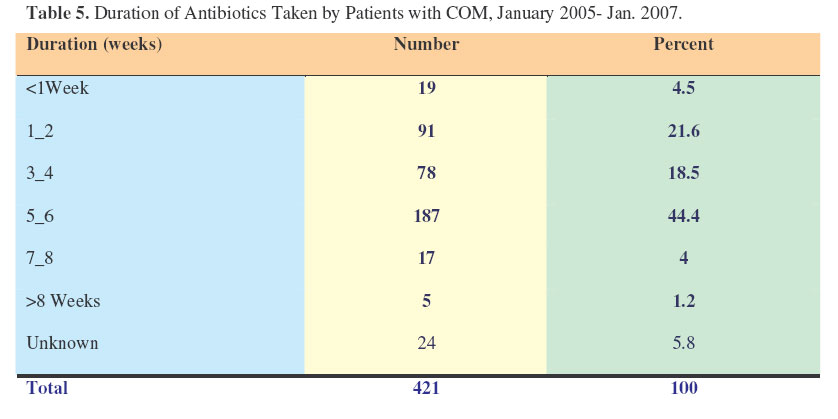
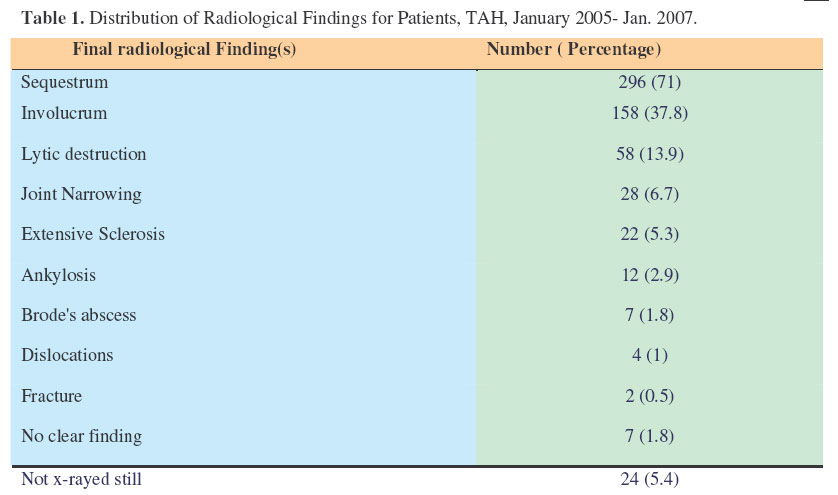
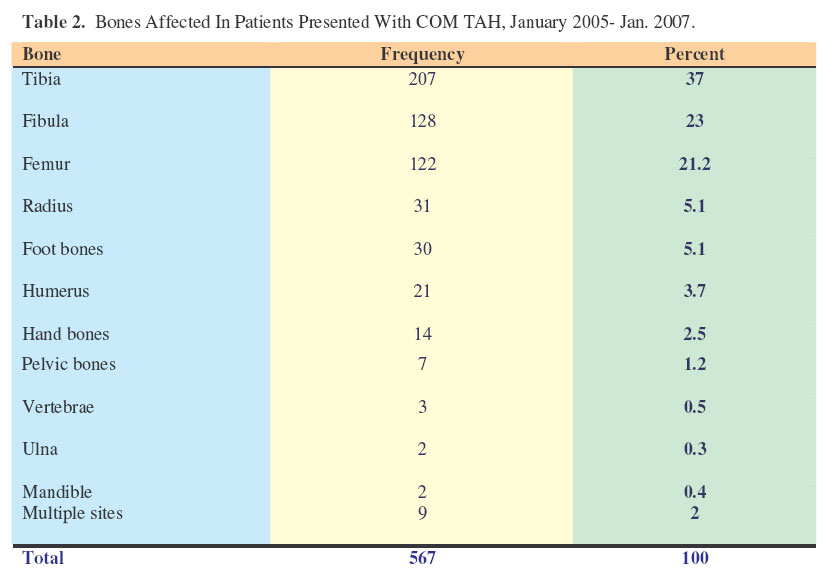
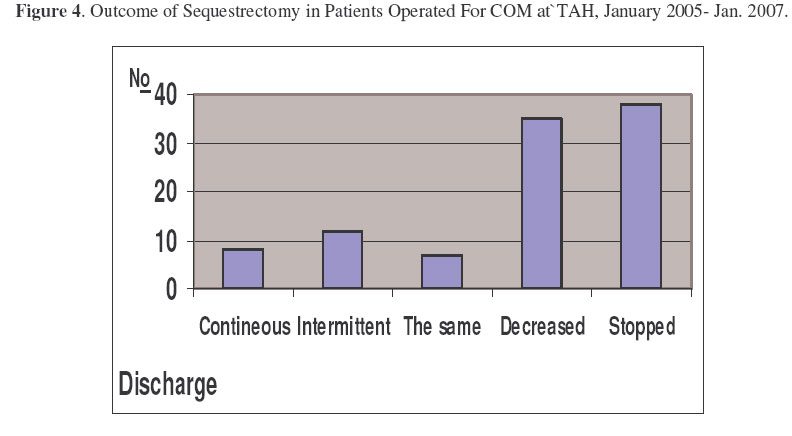
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 33-41 Chronic Osteomyelitis at Tikur Anbessa Hospital, Addis Ababa University, Ethiopia. Biruk, W.L. & Wubshet, K. Department Of Orthopaedics, Addis Ababa University, Correspondence to: Dr. Biruk WL. P.O.Box: 122201, Addis Ababa, E-mail= lbiruklw@yahoo.com Code Numbe: js07007 Background: Chronic osteomyelitis (COM) is a severe, persistent and sometimes incapacitating infection of bone and bone marrow. This prospective study at Addis Ababa University, Medical Faculty, Department of Orthopaedic Surgery, Tikur Anbessa Hospital was aimed at determining the pattern of chronic osteomyelitis and the out come of its management.. Introduction Chronic osteomyelitis (COM) is a severe, persistent and sometimes incapacitating infection of bone and bone marrow1 .It may occur spontaneously, follow inadequately treated acute osteomyelities (3-25%), trauma or surgery. Infection at the bone locus creates an increase of intramedulary pressure due to inflammatory exudates that strips the perosteum, leading to vascular thrombosis followed by bone necrosis and formation of sequestra. This dead bone is surrounded by thick relatively avascular granulation tissue which is hard to permit antibiotics. At the same time there is new bone, involucrum formation with multiple openings, cloacae, to discharge pus through sinuses. Even though this is a typical pathophysiology of Haematogenous osteomyelitis, post-traumatic COM also shares some but not all of these characteristics14 . The incidence of COM is very high in developing countries and is also increasing and its management is often difficult and imposing significant proportion to the scarce medical services in Africa4-6 . It accounts for some 30% of admissions to our Hospital. COM has different forms and Cierny-Madre’s classification, currently best used, incorporates both anatomic and physiologic parameters of the patient12 . Staphylococcus aureus has special receptors for adherence onto the bone; hence it is the major bacteriological ethiology17,30 . For late coming patients in Africa, diagnosis is not a challenge and basic haematological investigations are nonspecific20- 23 . Sinus discharge culture is misleading and proper specimen must be taken from the infected bone24,31 . For florid COM in Africa, plain film gives reasonable information, but sometimes other modalities of investigation may be necessary25-29 . One has to take care not to miss bone neoplasm and biopsy is still the gold standard32 .Treatment of COM is difficult, multifaceted and multidisciplinary33 . There are different methods of treatment used under different circumstances1-4 . Post traumatic osteomyelitis usually arises from open fracture and such a fracture needs serious attention34 .In African set up, where traditional healers may delay modern treatment and is associated with complications, public education may also help to decrease COM35 . Patients and MethodsThis prospective study included all the 442 patients with different forms of chronic osteomyelitis presenting to the Department of Orthopaedics in the two years study period, Jan. 2005 to Jan. 2007. A standardized pre-tested questionnaire which contains the study variables was used to interview the patients after getting their consents. Operated patients were followed with a separate questionnaire with additional variables. Diabetic and vascular foot-osteomyelitis patients were excluded because they were included in other study. Addis Ababa University, Tikur Anbessa (Black lion) Hospital (BLH) is a tertiary level teaching hospital of the Medical Faculty .The orthopaedic department is the only orthopaedic speciality-training department in the country. It gives four-year orthopaedic residency training for medical doctors. It has over 560 beds and receives referred and some directly visiting patients from all over the country. In total, 67 (12%) of the beds are allocated to Orthopaedic Department. Only 18 (27%) of the 67 beds are for paediatric patients. The Orthopaedic Department has a referral clinic (2 days), a Club Foot Clinic, Paediatric Clinic (2 days), Fracture Follow-up Clinic (4 days), Medico-legal Age Determination Clinic, three major and one minor operation days. It has units in other Hospitals in the capital and also gives services like percentage disability assessment and referrals to abroad. Diagnosis of COM was mainly clinical with an aid of some basic investigations. Chronic Osteomyelitis was defined as a persistent infection of bone and marrow with sign symptoms lasting more than six weeks. The disease was referred as ‘Multiple’ when more than one anatomic region was affected. The study was supported and followed by the orthopaedic department. Statistical analysis was performed by EpiInfo-2002 software. ResultsA total of 442 consecutive patients with chronic osteomyelitis (COM) were included. Males accounted for 336 (76%) of the cases. The mean age at the initial presentation was 18 years with a range of 1month to 84 years. The majority (68%) of patients came from rural areas. Discharging sinus was the commonest clinical presentation observed (411, 93%) followed by swelling (260, 59%), pain (240, 54%), limping (188, 42%), and limitation of movement (131, 30%). Squamous cell carcinoma was present in four patients (Figure 1). The disease started spontaneously in 70% (312) and it followed trauma in 27% (118). Tuberculosis osteotitis was proven in three of the suspected patients and the disease occurred post operatively in eleven patients (Figure 2). Compound fracture accounted for 93 (79%) of the post traumatic onset and the osteomyelitis followed simple fractures in 12 (10%) of the patients (Figure 3). More than half (230, 52%) of the patients visited bone setters in the course of their illness and “difficulties” at Hospitals were one of the main reasons (41, 18%) (Table 3). Only 21 (4.8%) of the patients did not take any antibiotic in the course of their illness and majority of those who took antibiotics had taken them for more than a month (Table 4 and Table 5). Seventy five (81%) of the patients with compound fractures initially visited a Hospital but were referred elsewhere due to lack of beds for admission. The commonest radiological finding seen was a sequestrum (189, 58%) and involucrum formation (174, 53.5%) followed by joint space narrowing (67, 20.6%) (Table 1).A quarter (117, 26.5%) of the patients were not initially x-rayed when referred to our Hospital and 296(67%) of them had no any laboratory investigations. ESR was more than 30mm/hr in 86% of the patients, there was Leukocytosis in 38% of the patient and 43% of the patients were anaemic (Haematocrit <30%). The commonest anatomical type noticed using Cierny-Mader’s classification was type III (273, 63%) followed by type IV (82, 19%). Thirteen patients were difficult to classify. More than half, (58.6%) of the patients came to the Hospital two years after the onset of the illness. Lower limb bones were the commonest affected (Tibia, 36%, fibula 22% and femur 21%)(Table 2). Nine of the patients had multiple bones affected and three of these patients agreed to HIV screening, all were positive.Swab culture was done in only half of the patients. The main isolate was Staph. Aureus and most of the organisms were resistant to the common antibiotics. Most of the patients (304, 69%) were waiting for surgery. Sequestrectomy had been done only in 73 (16.5%) of the patients and the discharge stopped in 38 (52%)(Figure 4). DiscussionThe predominantly male (76%) young (mean age 18 years) patients from rural areas (68%) in our study were similar to other findings in developing countries. Many of these were likely to be heads of households shouldering other family members, thus the disease has exponential damage on poor Africans who are cost sensitive. On our two years prospective study of COM at Addis Ababa University, discharging sinus was the commonest clinical presentation observed (411, 93%) followed by swelling (260, 59%), pain (240, 54%), limping (188, 42%), and limitation of movement (131, 30%).This is in agreement with most studies1,7,8,11-13 . Squamous cell carcinoma was present in four patients. Most of the sinuses were super infected as the majority of the patients appeared to Hospitals very late and sometimes after visiting traditional healers. The disease started spontaneously in 70% (312) and it followed trauma in 27% (118). Tuberculosis osteotitis was proven in three of the suspected patients and the disease occurred post operatively in eleven patients. Compound fracture accounted for 93 (79%) of the post traumatic onset and the osteomyelitis followed simple fractures in 12 (10%) of the patients. This is one of the potential areas where preventive measures can be taken. More than half (230, 52%) of the patients visited bone setters in the course of their illness and “difficulties” at Hospitals were one of the main reasons (41, 18%).It is distressing that 70% of emergency patients requiring urgent surgical admission had to be referred back elsewhere for lack of beds in our Hospitals-no wanders if patients look for other alternatives, like traditional bonesetters. One remedy may be to train bone setters35 . Only 21 (4.8%) of the patients did not take any antibiotic in the course of their illness before surgery, and majority of those who took antibiotics had taken them for more than a month. This we believe has no help except increasing resistance as the antibiotics could not penetrate the pathology17 . Seventy five (81%) of the patients with compound fractures initially visited a Hospital but were referred elsewhere due to lack of beds for admission and most of these patients will not get beds in the ‘other’ Hospitals too. Giving appropriate antibiotics to this patients may temporarily help34 . The commonest radiological finding seen was a sequestrum (189, 58%) and involucrum formation (174, 53.5%) followed by joint space narrowing (67, 20.6%).A quarter (117, 26.5%) of the patients were not initially x-rayed when referred to our Hospital and 296(67%) of them had no any laboratory investigations. ESR was more than 30mm/hr in 86% of the patients, there was leucocytosis in 38% of the patient and 43% of the patients were anaemic (Hematocrit <30%).This may affect to monitor treatment response during follow-ups and also the anaemia, as a reflection of malnutrition may impair healing21 . The commonest anatomical type noticed using Cierny-Mader’s classification was type III (273, 63%) followed by type IV (82, 19%). This is the currently accepted classification to plan management, but with plain films alone it is difficult to classify patients into types-I and II 12 . More than half, (58.6%) of the patients came to the Hospital two years after the onset of the illness. At any rate, they were very late and this makes treatment a challenge and the outcome will be very poor due to malnutrition and soft tissue contractures (32). Lower limb bones were the commonest affected (Tibia, 36%, fibula 22% and femur 21%). This is in consistent with many studies as the lower limb is more prone to injuries in our set-up29. Nine of the patients had multiple bones affected and three of these patients agreed to HIV screening, all were positive. Multifocal disease may be an indicator of failure of the immune system5. Swab culture was done in half of the patients. This is a useless practice except compromising patient’s money. Proper culture from the sequestrum should be done31 . The main isolate was Staph. Aureus and most of the organisms were resistant to the common antibiotics. Most of the patients (304, 69%) were waiting for surgery. Sequestrectomy only had been done only in 73 (16.5%) of the patients and the discharge stopped in 38 (52%).We feel this is not an adequate treatment as the treatment of COM is multidisciplinary, team approach and has different stages such as: complete excision of the necrotic bone, limb stabilisation, prolonged sensitive antibiotic therapy, obliteration of dead space and reconstructive surgery2-4, 33 . RecommendationsBased on our findings we recommend the following:
I dedicate this paper to my understanding,brilliant and tough wife, Lili. Dr. Stephen K. Wood and Anita, thanks for coming to Addis and editing this paper. Dr. Tessema and Dr. Birhanu of SSE, thank you for your persistent encouragement and appreciation. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07007f3.jpg] [js07007t2.jpg] [js07007t1.jpg] [js07007f4.jpg] [js07007f1.jpg] [js07007t5.jpg] [js07007f2.jpg] [js07007t3.jpg] [js07007t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}