 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
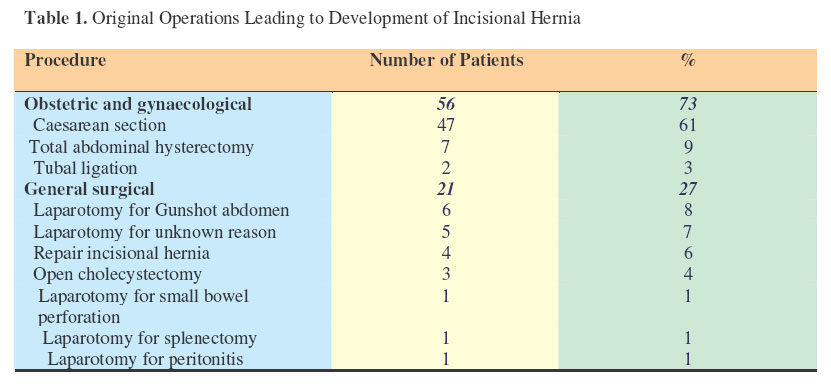
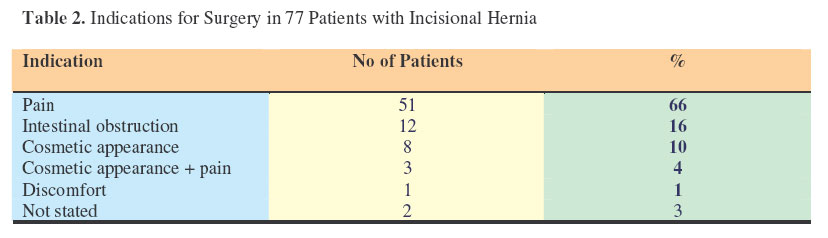
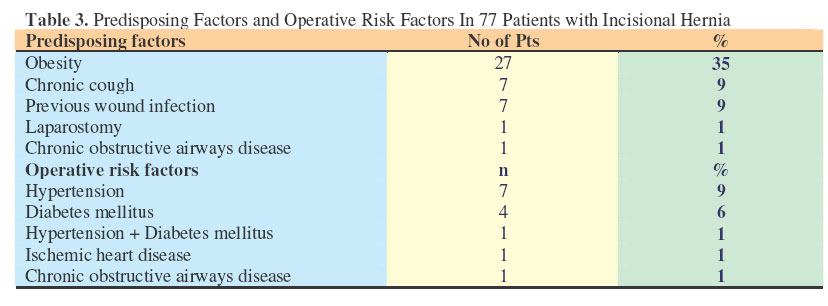
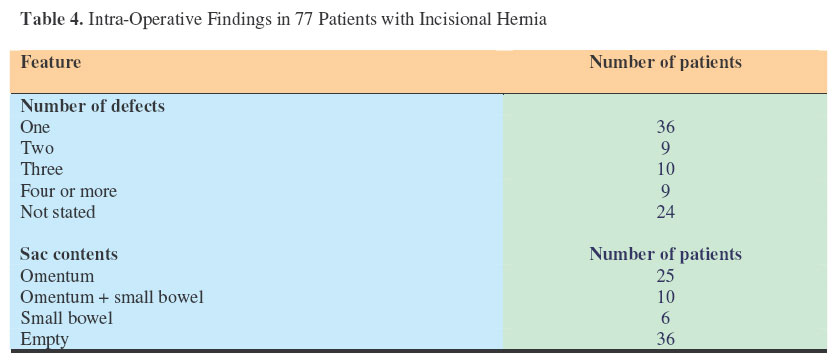
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 42-46 Incisional Hernia: Experience in a Single Surgical Unit Pillay, Y.; Naidoo, N. M. & Madiba, T.E. Dept of Surgery, University of KwaZulu-Natal and King Edward VIII Hospital, Durban, South Africa. Code Number: js07008 Background: Incisional hernias are a common problem in general surgery and they have a varied aetiology. The aim of this study was to document a single unit experience with the management of incisional hernias at King Edward VIII Hospital, Durban, South Arica. Introduction Incisional hernias are a common problem in general surgery. They develop in 2-11% of patients undergoing laparotomy1-3 . In 80-95% of patients, they develop within 6 months to 3 years after initial surgery 2,4 . Hernias that develop within three years of operation are more likely to be troublesome and larger in size than those that develop late5 . The common risk factors include multiple abdominal procedures, wound infection, chronic cough, obesity, emergency procedures, early re-operation and surgical technique1,3,6 . The aim of this study was to document our experience with the management of incisional hernias at King Edward VIII Hospital, Durban. Patients and Methods This was a prospective study of patients with incisional hernias in a single ward at a tertiary teaching hospital over a period of 41 months (January 2001 to May 2004). Demographic data, nature of original operation, intra-operative findings and procedure performed were all documented in a standardised proforma. Documented intra-operative information included the identification of the original suture, the number of defects and the type of repair done. There was selective mesh repair only if the defect could not be closed without tension. This was left to the preference of the surgeon. There was no standard protocol regarding repair and the type of repair was left to the preference of the treating surgeon. Generally a tissue repair was performed using loop nylon suture. Results A total of 77 patients were treated for incisional hernia during this period, of which 70 were female. Their mean age was 44.34 + 13.09 years (range 22-81). Previous operations leading to incisional hernia are shown in Table 1. In 73% of cases the previous procedures were gynaecological (inclusive of gynaecology and obstetrics). The period between original operation and the development of symptoms was between 1 month and 15 years. Indications for surgery are shown in Table 2 and predisposing factors and operative risk factors are shown in Table 3. Fifty three and 24 patients underwent elective and emergency surgery respectively. Table 4 shows patients stratified according to the number of defects and contents of the sac. One patient had a Richter’s hernia. The bowel was gangrenous in 3 patients. Tissue repair was undertaken in 74 patients (with loop nylon in 62, Polydiaxanone-S (PDS) in 9 and Polypropylene in 3) and mesh repair was undertaken in 3 patients. A drain was left in situ in 27 patients. A total of 13 patients (17%) developed complications; 7 (10%) developed wound sepsis. Five patients needed management in the ICU. Hospital stay was 8.13 + 10.72 days (range 2-93 days). Three patients died (4%), following emergency operations. One patient with asthma and chronic obstructive airways disease (COAD) developed wound dehiscence and required re-repair; the second patient with COAD had had intestinal obstruction for two months before admission to hospital; the third patient had gangrenous bowel at surgery. All three patients were ventilated postoperatively in the ICU and died from multiple organ dysfunction syndrome (MODS). Twenty-nine patients (38%) had left contact details. When contacted later, 7 (25%) of the 29 patients agreed to come in for further review (follow-up 6 months to 4 years). One had hernia recurrence and one patient was not satisfied with the result even though her repair was still intact. Both had had tissue repairs and were reviewed 4 years after surgery. The remaining five patients were satisfied with their repair. DiscussionIncisional hernias are a common problem in general surgery and they develop in 2-11% of patients undergoing laparotomy1-3 . While some studies have shown a male predilection1-3,6, others have found no sex predilection7. There was a female preponderance of 6:1 in this study. The aetiology of incisional hernia is multifactorial and, despite numerous predisposing factors, the underlying cause of the development of hernias seems to be of a biological nature4. An abnormal collagen metabolism has been ascribed an important role in the genesis of incisional hernia and the high recurrence rates after surgical hernia repair. It seems plausible that a mal-union occurs between the edges of the incised aponeurosis soon after operation and that the weak fibrous tissue forming that mal-union insidiously stretches, until the hernia becomes clinically detectable 8,9. Sepsis inhibits collagen synthesis resulting in slowing of epithelialization and wound contraction9. Although many predisposing factors for incisional hernia are patient related, some factors may be influenced by the surgeon in the prevention of incisional hernia. These include the type of primary closure, wound infection rate and materials used4. None of these factors were controlled or standardised in our study. The ideal suture material for closure of abdominal wound should have three important characteristics, namely retention of high tensile strength, monofilament structure so that bacteria cannot hide within any interstices and absorbable qualities so that the material is ultimately eliminated as a source of infection3. Experimental research has shown that one year after laparotomy the abdominal fascia retains only 70% of its original tensile strength9. Polyglactin (Vicryl) and Polyglycolic acid (Dexon) are degradable and they have the advantage of disappearing after 75 days but they have no tensile strength after 30 days. Polydiaxanone-S (PDS) is a monofilament suture having the advantage of nylon and polypropylene with smooth surface which slides easily through the tissues4. PDS is only absorbed after 180 days and retains 70% of its strength after 3 weeks; it seems to be associated with a lower rate of incisional hernia9-11 . Studies comparing wound closure by absorbable and non-absorbable sutures have shown no difference in the overall incidence of incisional hernia 9 . In a meta-analysis by Hodgson et al 12 incisional hernia was 32% less frequent with non-absorbable sutures compared to absorbable. Furthermore non-absorbable sutures had an increased rate of cutaneous sinuses and wound pain. In abdominal wound closure continuous suture closure is as effective and as safe as interrupted suture closure with the advantage of being more expeditious4,11,13 . There is evidence to suggest that layered closure is associated with increased risk of infection, hernia and dehiscence compared to mass closure14 . Weiland et al14 also recommend that non-absorbable sutures should be used for continuous closure and that absorbable sutures should be favoured for interrupted closures. In many cases with hernias of small to moderate size fascial defects, closure can be achieved by apposing the edges of the fascia and closing the wound in a continuous mass closure1,3,9 . The likelihood of adequate and long-lasting repair can be increased by adherence to specific surgical principles1,3 . Sutures are best placed about one centimetre apart in order to provide for incorporation of healthy fascia on either side of the edge and avoid protrusion of abdominal contents through the fascia3 . Problems with the absorbable suture such as sinus formation or infection may have been the overriding concerns that have resulted in the use of non-absorbable suture4 . When the defect is sufficiently large to preclude the use of simple closure a number of other primary repairs have been proposed including relaxing incisions and prosthetic mesh repairs1,3 . The use of synthetic mesh in incisional hernia repairs increased dramatically in the 1990s15 . Some studies seem to suggest that mesh repair is superior to suture repair with regard to recurrence16 , others contend that there is no one technique that best procedure for all patients17 . It is interesting to note that the major operations leading to incisional hernias were gynaecological in this series. This is difficult to explain. It would be unfair to suggest that the gynaecological nature of the operation predisposes to incisional hernia. Many factors need to be considered such as wound factors, patient factors, tissue factors and type of closure during the previous operation. A previous suture could not be identified in over half of the patients suggesting that an absorbable suture might have been used in the original operation. Up to 19% of hernias are preceded by wound infection1,3,6,9, which is much higher than the 7% observed in this series. The complication rate was 17% with 10% wound sepsis rate and there was no seroma. These figures differ from those in the literature where seroma formation is reported in 3-6% 2,18 and wound infection in 1% 18 . There was no seroma formation in this series but superficial wound infection occurred in 10%. It is worth bearing in mind, however, that this study reflects a single unit experience and the findings cannot be generalised. Incisional hernia repair is associated with cumulative rates of re-operative repairs15 and recurrence rate after repair has been reported at 10-50%1,3,9,18 . Interestingly with the advent of prosthetic meshes being used for incisional hernia repair, the recurrence rate has dropped to about 5% 1,15,19 . Unfortunately follow-up was very poor in this series. A large number of our patients are from rural areas and transportation is both unreliable and expensive. Furthermore patients do not present to hospital unless they are having problems. Sometimes patients accept a small recurrent hernia as normal and do not present to hospital for medical attention. Conclusion Most incisional hernias in this series followed gynaecological surgery. There was no evidence of a non-absorbable suture having been used at the original operation in over half of the patients. Whatever material or technique is used for abdominal wall closure it cannot and should not be a substitute for meticulous technique. This study was unable to elucidate clearly the recurrence rates because of poor follow-up. Now that meshes are being used increasingly in our unit further prospective studies need to be done to assess recurrence rates. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07008t1.jpg] [js07008t4.jpg] [js07008t2.jpg] [js07008t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}