 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
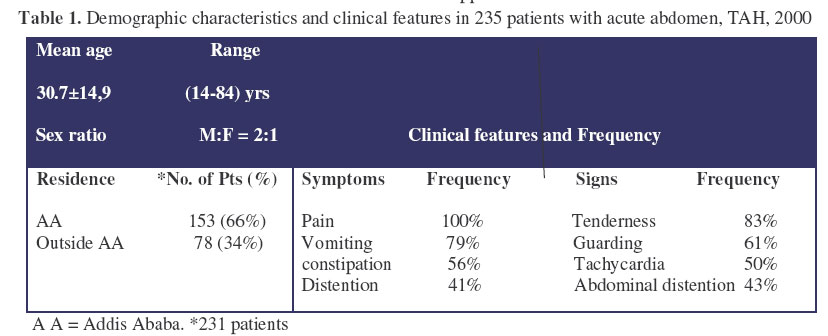
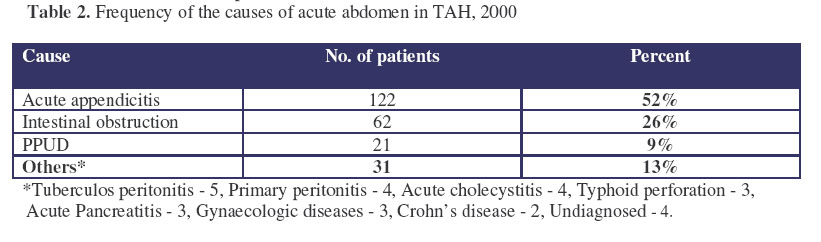
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 47-52 Pattern of Acute Abdomen in Adult Patients in Tikur Anbessa Teaching Hospital, Addis Ababa, Ethiopia. Kotiso1, B. & Abdurahman2, Z. 1Associate Professor of Surgery, AAU, Medical Faculty, Department Of Surgery, 2Assist.Professor of Surgery, Gonder University, P.O.Box 196 E-Mail :Zekia2001@Yahoo.Com Code Number: js07009 Back ground: Surgical acute abdomen is one of the commonly encountered emergency in the practice of General surgery but there is no much study regarding the magnitude and its pattern in Ethiopia at large and in Tikur Anbessa Hospital (TAH) in particular. This study was aimed at assessing the magnitude, pattern and outcome of surgical treatment of acute abdomen in TAH Introduction Acute abdomen is defined as a sudden onset abdominal disease condition which often requires an immediate surgical intervention. The causes of acute abdomen are several and their relative incidence varies in different populations. Several factors are described to be responsible for these differences. Socioeconomic factors and diet have mostly been incriminated to be responsible for the observed differences1,2,3 . Intestinal obstruction has been the leading cause of acute abdomen in several African countries whereas acute appendicitis is the most frequently seen cause in the developed world2,4,5,6 . The leading causes of intestinal obstruction in Africans have mostly been hernia and volvulus whereas adhesions are most frequent in the developed world6-12 . There are, however, some African studies which are pointing to a change in these established patterns13, 14 . In Ethiopia, very little is known about the general pattern and the relative incidence of the causes of acute abdomen. This study was conducted with the aim of assessing the magnitude, pattern and out come of surgical treatment of acute abdomen in Tikur Anbessa Teaching Hospital and compare it with other studies in the country, Sub Saharan Africa and also the developed world. The study is believed to have epidemiological and clinical benefits and would also serve as a base for other studies. Patients and Methods Tikur Anbessa Hospital (TAH) is a University hospital in Addis Ababa, Ethiopia, with a capacity of 500 beds. The study is a retrospective clinical based type covering a period of one year from January 1st to December 31st 2000. The daily admission records were used to retrieve patients’ records. Those cases admitted to the surgical wards with a clinical diagnosis of acute abdomen were included in the study whether they were operated or not. Patients with protracted course of illness with acute exacerbation were included in the study realizing the acute on chronic process of their condition. Pediatric patients aged 13 years and below were excluded from the study. There were 276 adult patients who were admitted with a working diagnosis of acute abdomen. Of these, the records of 235 patients were retrieved which formed the basis of this study. Data concerning socio-demographic characteristics, duration of illness, visit to other health institutions, presenting symptoms and signs, operative findings, post operative course and outcome were extracted and filled in a previously prepared protocol sheet. It was then analyzed using EPI-6 statistical software. Results A total of 587 adult surgical emergency operations were performed during the study period. The number of patients admitted with the diagnosis of acute abdomen was 276 of whom the records of 235 patients were retrieved for analysis making a retrieval rate of 85%. Two hundred and fourteen (36.4% of the emergency operations) of these were operated, 15 were managed conservatively (cases of appendiceal mass, post operative adhesion and acute pancreatitis) and 6 died before surgery. Of those whose addresses were identified, 153 (66%) were from Addis Ababa (A.A) and 78 (34%) were from out side A.A. Their age ranged from 14 to 84 (mean = 30.7 ± 14.9) years. One hundred and fifty five were males and 80 were females with a male to female ratio of 2: 1. The duration of illness at presentation ranged from 6 hours to 21days (mean = 4.6 days), and 169 (72%) of the patients had visited other health institutions once or more before their presentation to our hospital. Abdominal pain and vomiting were the most frequent symptoms (100% and 79% respectively) whereas tenderness and guarding were the most frequent clinical signs found (83% and 61% respectively) (Table 1). As is shown on Table 2, the most common cause of acute abdomen was acute appendicitis found followed by intestinal obstructions 62(26%) and PPUD 21(9%). Acute appendicitis accounted for just over half of the cases 122 (52 %), of whom 81 (67%) were males and 41 (34%) were females (M: F =2:1). The majority of the cases were in their second and third decades of life. Four patients with acute appendicitis had died. Table 2. Frequency of the causes of acute abdomen in TAH, 2000
*Tuberculos peritonitis -5, Primary peritonitis -4, Acute cholecystitis -4, Typhoid perforation -3, Acute Pancreatitis -3, Gynaecologic diseases -3, Crohn’s disease -2, Undiagnosed -4.
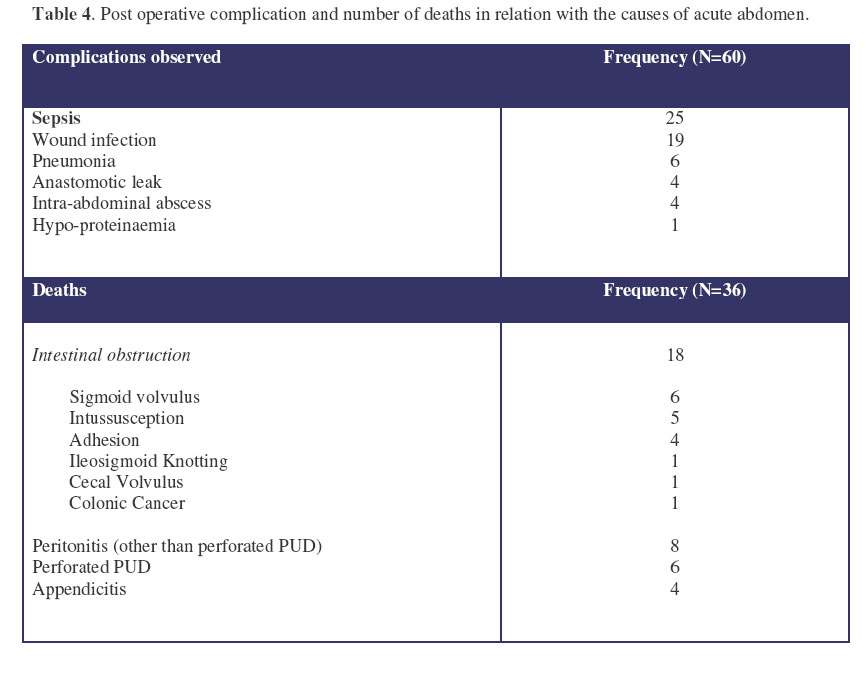
Table 4. Post operative complication and number of deaths in relation with the causes of acute abdomen.
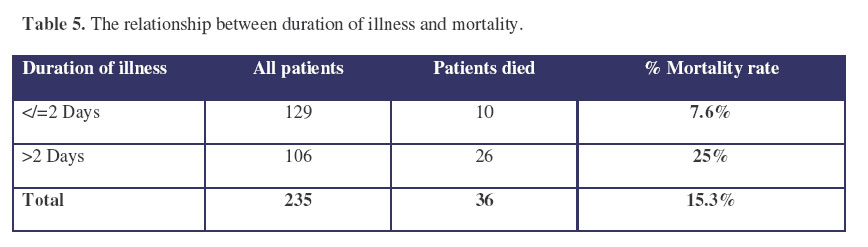
Table 5. The relationship between duration of illness and mortality.
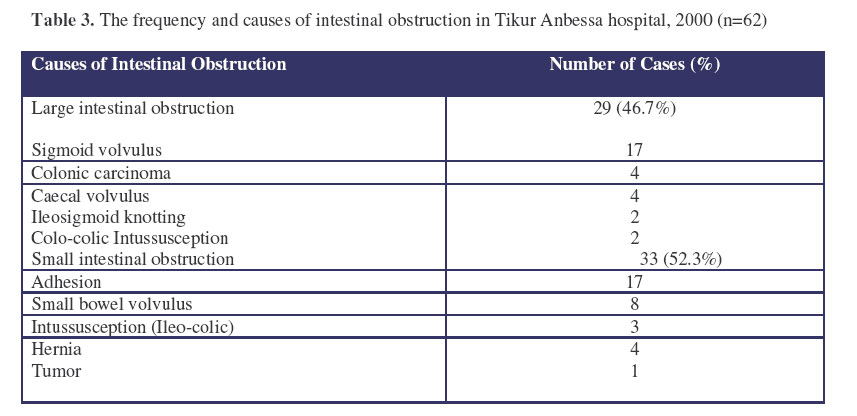
The frequency and causes of intestinal obstruction are shown on table3. Small bowel obstruction due to adhesion and sigmoid volvulus were the leading causes of intestinal obstruction each accounting for 27% (N=17). The relative frequency of the causes of small bowel obstruction is also shown on table 3. The mean duration of presentation was 8 days. Twenty-four were males and 15 were females. The mean age of the patients was 31.5 years and two-third were from outside of A.A. Seven out of the 33 patients with small bowel obstruction had died giving a mortality rate of 21.2%. Adhesions were the most frequent cause of small intestinal obstruction (17/33). Nine were males and 8 were females. Ten were from outside A.A and 12 had previous surgery. Four were managed conservatively and 13 were operated out of which four had died. There were 8 patients with primary small bowel volvulus of whom 6 were males and 2 females; seven were from outside of AA, and all had recovered. There were 3 cases of ileo-colic primary intussusception that came from outside of A.A. and presented very late. All of them succumbed after surgery. Sigmoid volvulus was the leading cause of colonic obstruction (17/29). Fourteen were males and 3 were females. Their ages ranged from 40-78 years and the mean age was 58 ±11.4 years. Eight were from A.A and 9 from outside of A.A. The average duration of illness at presentation was 4.5 ±2.1 days. Seven had simple volvulus and 10 gangrenous. Three of the patients with gangrenous sigmoid volvulus died before surgery and two others died after surgery. One of the patients with simple sigmoid volvulus died after simple derotation by laparotomy. In total, 6 (35%) patients with sigmoid volvulus died (Table 4). PPUD was the third most common cause of acute abdomen identified accounting for 21 (9%) of the cases. Sixteen were males and 5 females. Their age ranged from 19 -64 (mean = 37.4 ± 13.9) years. Preoperative x-ray was done in 13 of these patients and free air under diaphragm was found in only 7. Three had multiple air fluid levels and 3 had normal x-rays. All the patients were operated and simple closure with Omental patch was done. Six (28.6%) of these patients had died. Table 4 shows the post operative complications and the number of deaths in relation with the causes of acute abdomen. There were 60(28%) cases that developed post operative complications. Sepsis was the most frequently identified complication in 25 (12%) followed by wound infection in 19 (9%) and pneumonia in 6 (3%). Overall, 36(15.3%) of the 235 patients who were admitted with the diagnosis of acute abdomen died. The mortality was very high (25%) in those with late presentation as compared to those who came relatively early taking two days as a cut off point (Table 5). Of the 214 patients who were operated, 30 died postoperatively accounting for an operative mortality rate of 14%. DiscussionThere are very few studies done on the general pattern of acute abdomen in Ethiopia12,16and few studies on specific causes of acute abdomen 7,8,9,17,21 . In this study, acute abdomen accounted for 36.4% of surgical emergency procedures. The male to female ratio was 2:1 and majority of patients were in their 2nd and 3rd decades of life, which was in agreement with previous studies done in the country and other African countries 11,12,13,16. There are no studies in Ethiopia describing the clinical presentation of patients with acute abdomen so far. All of our patients had abdominal pain as a presenting symptom followed by vomiting in 78%. Abdominal tenderness and guarding were the leading clinical signs which could be explained by the frequent encounter of acute appendicitis and late presentation. Acute appendicitis was found to be the leading cause of acute abdomen in our study. This is in contrast to the study done in Yirgalem, southern Ethiopia12 and some other African studies2,5,6 in which intestinal obstruction was the leading cause. However, appendicitis was found to be the leading cause in another study done in Nazareth, central Ethiopia16, and in Nigeria by Ajao14 and Zaire by Okoro15 . Two third of the patients in this study were from Addis Ababa, the capital city, which might be a reason for the high incidence of appendicitis as appendicitis has been reported to be more common in urban dwellers18,21 , but a true increment in its incidence is the likely reason as has been described by Ajao14, who has reported a change in the pattern of acute abdomen in Africa from one dominated by intestinal obstruction to a one dominated by appendicitis. The majority of the cases with acute appendicitis were in their second and third decades of life with male to female ratio of 2:1 which agrees with other studies16, 17,18 . Intestinal obstruction was the next most common cause of acute abdomen. The leading causes of intestinal obstruction in this series were sigmoid volvulus and small bowel adhesion each constituting 27.4%. The number of patients with sigmoid volvulus might have been increased if cases of sigmoid volvulus which were managed as an out patient by simple rectal tube deflation were included. This is in agreement with other studies done in the central and northern part of Ethiopia16,20 which have shown that sigmoid volvulus was the leading cause of intestinal obstruction. Studies done in the southern part of the country, however, had shown that small bowel volvulus was the leading cause of intestinal obstruction8, 9,12 . Adhesions were found to be the most frequent causes of small bowel obstruction in this study, which is in contrast to other studies that have been done in central and southern Ethiopia and neighboring Kenya8,9,10,12 , where small bowel volvulus was the leading cause of small intestinal obstruction, but in agreement to studies done in Nazareth, Ethiopia16 and in Nigeria by Adesunkanmi13 . Adesunkanmi has reported the changing pattern of intestinal obstruction from hernia, which has been the most frequent cause of small bowel obstruction in several African countries6,11,22 to a one dominated by adhesions. Most patient with small bowel volvulus were males from outside A.A which agrees to the fact that this problem is common in farmers7. There were 5 patients with primary adult intussusceptions: a condition which is very rare in the western world. All of them have died postoperatively, which could be described by the very late presentation (over three weeks) of these patients. PPUD ranked the third (9%) as a cause of acute abdomen which is in contrast to Zelalem’s report of only 2.2%12 . In this series the mortality of patients with acute abdomen treated surgically was 14%, which correlates to that of Datubo and Zelalem (13.3%) and (13.5%) respectively11,12 . The fact that majority of our patients consist of appendicitis with relatively low mortality rate of 3.2% has definitely underestimated the mortality rate. The mortality rate of 21.2% for small bowel obstruction, 35.2% of sigmoid volvulus and 28.5% of PPUD is very high. In this study the duration of illness was found to be strongly associated with the mortality rate. Patients who presented within two days of their illness had a mortality rate of 7.6% where as those who presented later than two days had a mortality rate of 25%(statistically significant p<0.005). The reason for late presentation to the institution delivering the surgical treatment needs to be studied further. The fact that majority (72%) of the patients had visited different health institution once or more, may indicate lack of appropriate institution or surgeon to handle acute abdominal situation which in turn might have played a role in the delay. Moreover a sizable number (34%) of the patients had come out of AA which could also explain the late presentation either due to lack of transport or little awareness to the acute abdominal situation. Conclusion Acute abdomen is a commonly encountered condition accounting for 36.4% of the surgical emergency procedures done in the department. There is some indication that the pattern of acute abdomen might be changing in the tropical African population, at least in the urban setting, with a tendency towards predominance by acute appendicitis and intestinal adhesions, a trend already started to be observed by some authors: Adesunkanmi13 and Ajao14. The overall mortality rate of 15.3% and post operative hospital mortality rate of 14% may be unacceptably high. Early diagnosis, adequate preoperative resuscitation and proper post operative care would help to reduce the observed high mortality. This could be achieved by increasing public awareness on clinical features of acute abdomen as well as by improving the knowledge of mid and lower level health professionals on the diagnosis, resuscitation and importance of early referral to higher center. Moreover, health facilities capable of handling patients with acute abdomen should be available within the reach of the community. AcknowledgmentWe are very much grateful to all who took part in the management of the patients. Our gratitude goes to the Hospital administration for their permission to use the records. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07009t4.jpg] [js07009t2.jpg] [js07009t5.jpg] [js07009t1.jpg] [js07009t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}