 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
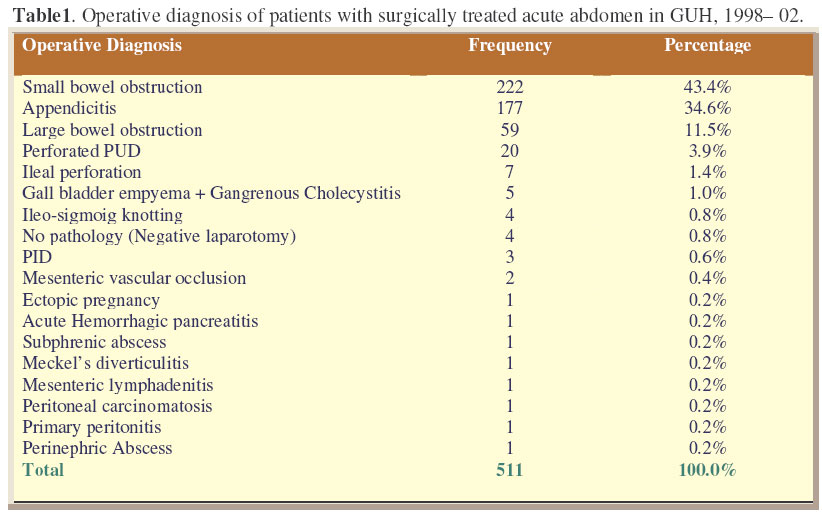
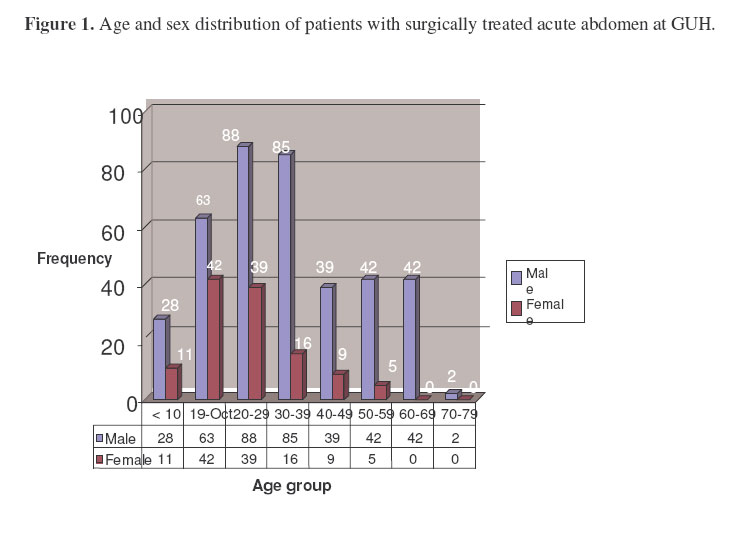
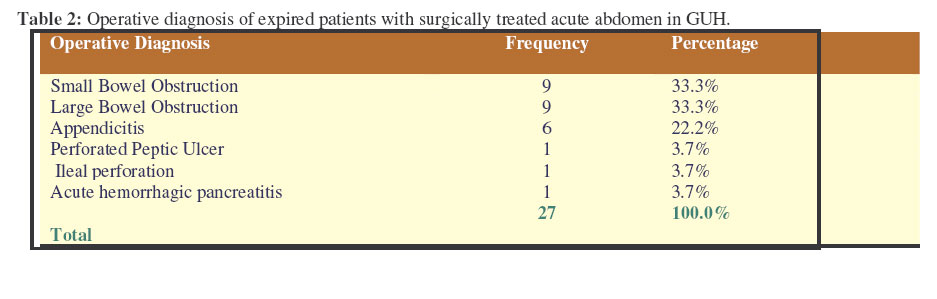
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 53-57 Surgically Treated Acute Abdomen at Gondar University Hospital, Ethiopia. Tsegaye1, S.; Osman2, M. & Bekele3, A. 1School of public Health, University of Gondar, 2Associate Professor of Surgery, University of Gondar,Ethiopia, 3Lecturer of Surgery, University of Gondar, Ethiopia Code Number: js07010 Background: Acute abdomen is an acute onset of abdominal disease entities that require immediate surgical intervention in most of the cases. The numbers ofresearches done on acute abdomen in general are Very few in Ethiopia. The main objective of this study was to document the burden of acute abdomen in general and the outcome of emergency laparotomy Introduction disease entities that require immediate surgical intervention in most of the cases. The causes are several with variable incidence in different populations. There may be a variety of reasons for these differences and for the outcome of the interventions. Though the causes are various, the commonly observed ones are few in number. Sigmoid volvulus is reported to be the commonest cause of emergency admissions with intestinal obstruction in Gondar University Hospital1,2 . The leading cause of acute abdomen in several African countries was intestinal obstruction, whereas acute appendicitis is top in the list in some studies3, 4, 5,6 . Of the major gastrointestinal disorders, acute appendicitis was the most common condition, accounting for one third of the cases in Black Lion Hospital7 . The presentation of different causes of acute abdomen overlap but there are some signs and symptoms that may help to narrow the differential diagnosis. The most common symptoms were abdominal pain and vomiting whereas tenderness and guarding were the most frequent clinical signs8. The numbers of researches done on acute abdomen in general are very few in Ethiopia. This study was conducted in Gondar University Hospital, North West Ethiopia, to investigate the pattern and burden of acute abdomen in general, factors attributable to the outcome of emergency laparotomy, and to get base line information to design a general management protocol for acute abdomen and further study. Methods Gondar University Hospital is located in the North West part of Ethiopia about 750 Km from the capital, Addis Ababa. It is a central referral Hospital for the north Gondar administrative region and the residences around. The hospital has about 370 beds of which more than 100 beds are used for surgical patients. The data was collected retrospectively from patient charts using a datasheet designed for this purpose. The variables included in the data are sociodemographic characteristics, surgical history, findings at presentation, operative and postoperative conditions. Charts of Patients operated for non-traumatic acute abdomen from 1998 to 2002were retrieved. Data were entered to EPI INFO 2004 version 3.2.2 statistical soft ware. Results A total of 4,978 surgical operations were performed in four years from the beginning of September 1998 to the end of August 2002. Of these 1179 (23.7%) were laparotomies for both elective and emergency cases. Emergency laparotomies for non-traumatic acute abdomen were 511 (43.3% of all laparotomies and 10.3% of all surgeries). The leading operative diagnoses were small bowel obstruction (SBO), appendicitis and large bowel obstruction (LBO) (Table 1). Of the 511 patients, 389 (76.2%) were male and 122 (23.8%) were females (M: F=3.2:1). Two hundred ninety seven (58.2%) were rural dwellers and 214 (41.8%) lived in urban areas. Seventy-two of the women were urban dwellers (59.2%). M:F ratio of rural dwellers was 5.3:1 whereas the ratio was 1.9:1 for urban areas. The mean age was 32 years. All the 511 records, of which 290 (56.8%) had adequate information for further analysis, were retrieved. However, the age and sex comosition, distribution of residence and the diagnosis pattern were identical between included patients for analysis and excluded ones. All patients (100%) had abdominal pain, 266(90.3%) had vomiting, 162 (55.9%) had constipation, 169 (58.3%) had abdominal distension. The median duration of illness was 72 hours with 75%of the patients presented with 5 days (120 hours) complaint. Ninety nine of the patients (34.1%) had longer than 72 hours duration of presenting complaint, 35 (35.1%) of which developed postoperative complication. One hundred thirty seven (47.2%) of the patients came to hospital earlier than 72 hours, and only 21(15.2%) of them developed postoperative complications. One hundred forty three (49.3%) of patients had signs of peritonitis, 76 (26.2%) were having localized peritonitis and 67(23.1%) presented with generalized peritonitis; 147 (51.7%) did not have sign of peritonitis at all. Thirty three (49.3%) of patients with generalized peritonitis developed postoperative complications. However only 46 (18.6%) of the cases with out generalized peritonitis developed postoperative complication. One hundred fifty two (52.4%) of the records showed a mean Haematocrit of 40.4 + 6.5. Two hundred forty two (83.4%) of the patients received antibiotics. One hundred ninety three (66.6%) had preoperative antibiotics, 81(27.9%) had antibiotics intraoperatively and 196 (67.6%) had antibiotics post operatively. Five (1.8%) had a single antibiotic, 41 (14.1%) had two antibiotics. One hundred ninety six patients (67.2%) received three antibiotics. Overall transfusion rate was 14.5% (42 patients were transfused with fifty-six units of blood). Seventy-seven (26.6%) of operated patients had early (in-hospital) postoperative complications. The median first postoperative complication detection time was the fourth postoperative day.The median hospital stay was 8 days. Seventy seven (55.6%) of the patients among those with less than 72 hours presentation-time stayed for 8 days or less in hospital. However, 66 (66.7%) of patients with presentation time longer than 72 hours stayed more than 8 days in Hospital. Twenty-seven of the patients (9.3%), twenty males and seven females, died. The average hospital stay of patients who died was 5.7 days. The median was 3 days. The mean age of patients who died was 41.5, and the median was 45. Ninety-eight patients (33.3%) had follow-up after discharge from hospital. Fourteen had developed long-term complications. Incisional hernia was the commonest complication found in those patients with long-term follow up. DiscussionA total of 4,978 surgeries were performed in four years from the beginning of September 1998 to the end of August 2002. Nearly a quarter of the operations (23.7%) were laparotomies for both elective and emergency cases. A total of 511 of the laparotomies were on emergency bases for non-traumatic acute abdomen, (43.3% of all laparotomies and 10.3% of all surgeries). Small bowel obstruction (43.4%), acute appendicitis (34.6%) and large bowel obstruction (11.5%) were the commonest three indications for non-traumatic emergency abdominal surgeries respectively. In a study done in the same hospital the commonest cause of intestinal obstruction was sigmoid volvulus1,2 . Our study put large bowel obstruction as the third commonest cause of operated acute abdomen. This difference is due to the fact that only acute abdomens operated on emergency basis were included in this study, excluding patients with sigmoid volvulus managed by rectal tube deflation and elective surgery. Of the 511 operated cases, 290 (56.8%) charts of patients had adequate information to be included in the study for further analysis. The charts of excluded patients were separately analyzed on their available information and the analysis found the age, sex and settlement distribution pattern, and the frequency of operative diagnosis were identical to those of included patients There are few studies of acute abdomen in Ethiopia9. Studies on particular causes of acute abdomen are also few3,4,5,6,10,11 . The clinical parameters of acute abdomen have not been well described and analyzed in Ethiopia. Males were more affected more commonly than females, with M:F ratio of 3.2:1. The mean age was 32.8 years. The male dominance is similar to other studies in Ethiopia but the age seems slightly older9. This may be due to the difference in pattern of cause of acute abdomen between the study areas. In this study, the leading cause of surgically treated acute abdomen was intestinal obstruction. This is similar to the study done in Yirgalem, Southern Ethiopia1 and some other studies in Africa3,4,12 . However, appendicitis was found to be the leading cause in studies in Nigeria and Zaire8, 13 . The majority of the patients were from rural areas (58.2%). However, the sex significantly differed by place of residence (X2= 12.74, p=0.0017). The male to female ratio among urban dwellers was 1.9:1 but it was 5.3:1 in rural areas. Moreover, the majority of the females operated for acute abdomen were from urban areas (59.2%). However, the general sex ratio in Ethiopian context is almost one to one14,15 . Though acute abdomen was more common among males, females from rural communities seem not to present to tertiary care health institutions compared to their male counter parts. This might be due to different reasons including women’s status in the community, their educational and economical capabilities which need to be addressed with other studies. Abdominal pain (100%), Vomiting (90.3%), abdominal distention (58.3%) and constipation (55.3%) were the commonest symptoms in patients with acute abdomen. The median duration of presenting complaint was 72 hours. Prolonged duration of presenting complaint was associated with increased occurrence postoperative complications and prolonged hospital stay (p=0.0395, p=0.000189). Nearly half of the patients (49.3%) had signs of peritonitis. Presence of generalized peritonitis was associated with increased occurrences of early postoperative complications and mortality compared to localized peritonitis (p=0.0008, p=0.0388 respectively). Antibiotics were administered for most of the patients (83.4%). Majority of the patients took Triple antibiotics (Ampicillin, chloramphenicol and Gentamycin). More than a quarter of surgically treated acute abdomen patients had one or more immediate postoperative complications. The three commonest immediate postoperative complications other than death were wound infection (20.6%), sepsis (17.6%) and pneumonia (9.9%). The median postoperative day to detect the first postoperative complication was the 4th post op day. Late detection of first post operative complication was associated with increased mortality (p=0.0016). Lower Haematocrit was associated with increased occurrence of early postoperative complications and deaths (p=00.0095, p=0.0065 respectively). The overall mortality rate of emergency surgically treated acute abdomen was 9.3% which is lower than the study done in Yirgalem (13.5%) and Datubo (13.3%) (11,12). The median hospital stay of expired patients was three days which is lower than that of eight days for the whole surgically treated acute abdomen. The median age of the expired patients was 45 years, older than median age of the studied population 30 years. Older age was significantly associated with mortality (p=0.006). About two thirds (66.6%) of the patients who died were operated for intestinal obstruction. Of the patients dying with large bowel obstruction, seven (77.8%) had gangrenous sigmoid volvulus and two (22.2%) had sigmoid tumor. Three (33.3%) of the patients who died of small bowel obstruction had intussusceptions, three (33.3%) had postoperative adhesion and two (22.2%) had gangrenous volvulus, the remaining one (11.1%) had internal hernia. Four (66.7%) of the expired patients with appendicitis had generalized peritonitis. In conclusion, this study has shown what the commonest symptoms of acute abdomen are and that the outcome of emergency laparotomy may be affected by different factors. Some of these factors were duration of illness, age, presence of peritonitis, Haematocrit level and complication detection time. Since the management is almost the same for almost all causes of surgical acute abdomens, the above-mentioned factors should be given due attention in handling such patients. The reasons for low appearance of rural female dwellers to better health care centers need to be investigated AcknowledgementsThe authors sincerely acknowledge the Gondar University Hospital and all health professionals who took part in the management of the patients. Reference
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07010t1.jpg] [js07010f1.jpg] [js07010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}