 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
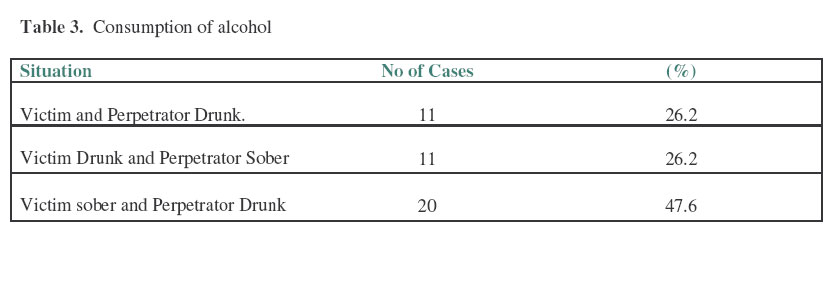
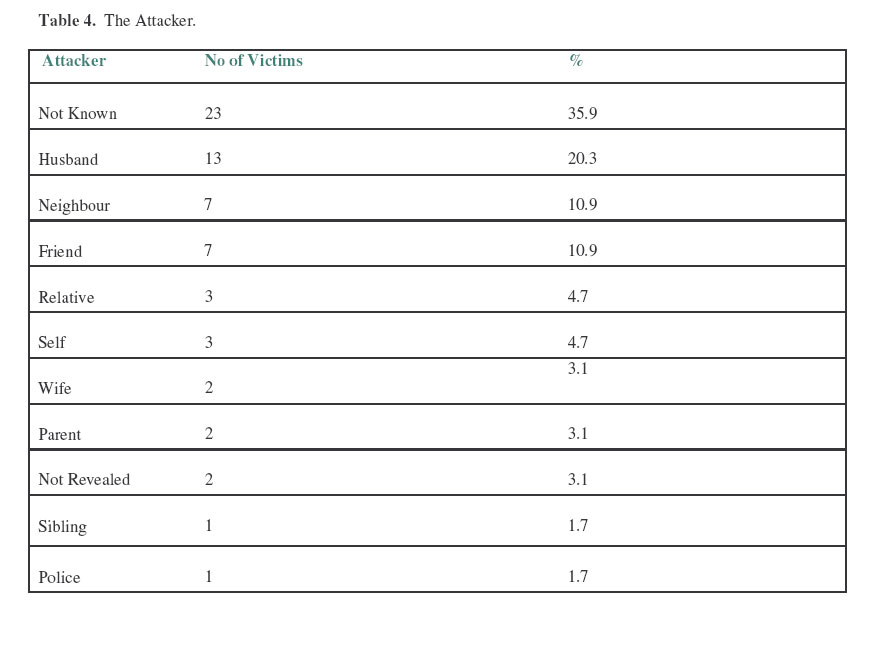
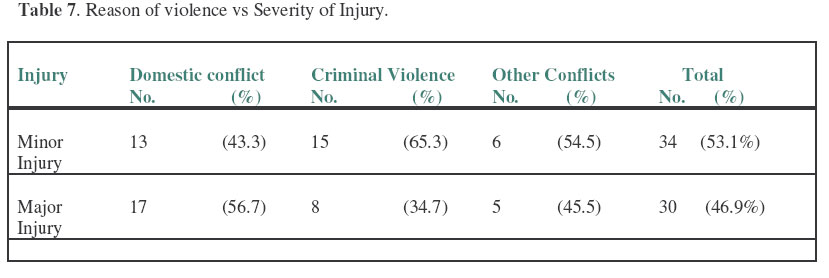
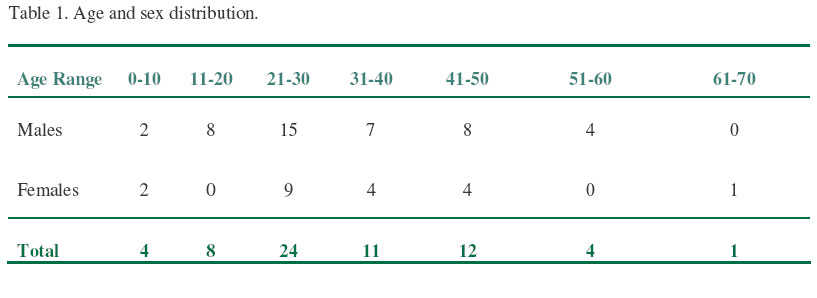
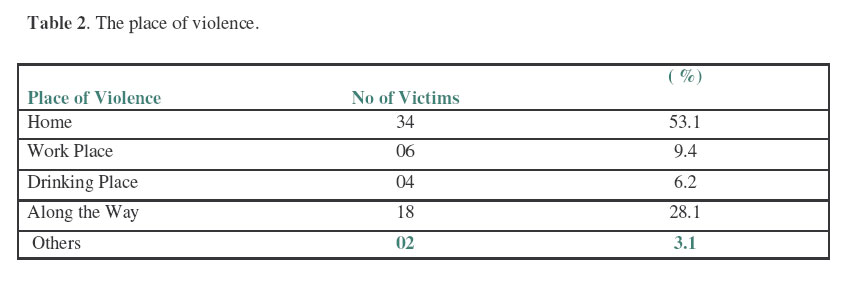
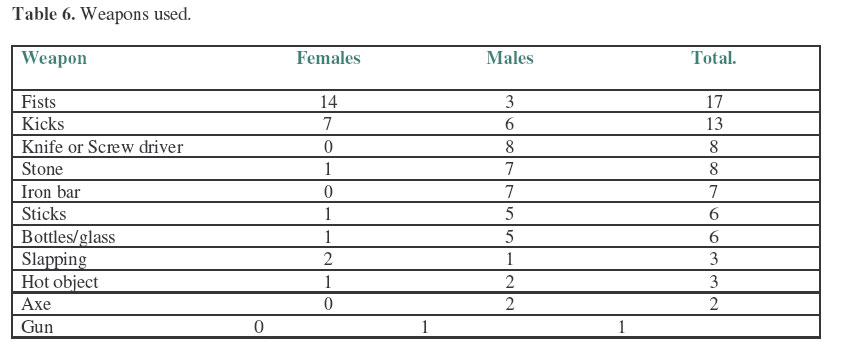
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 68-73 Admisions for Physical Violence in Chingola –Zambia. Mugala1, D.D. & Imataa2 , D. 1Consultant Surgeon, 2Theater Nurse Nchanga South Hospital Code Number: js07013 Background: Violence is a social disease that plagues all societies. Each society has its own form of violence. No doubt Chingola which is a growing mining town of over 200,000 people has its own pattern of violence and here is presented the pattern of physical violence in our town. This was a prospective study aimed at studying the prevalence and pattern of serious physical violence in Chingola. Introduction Violence is a social disease that plagues all societies. Each society has its own form of violence. No doubt Chingola which is a growing mining town of over 200,000 people has its own pattern of violence and here is presented the pattern of physical violence in our town. The aim was to study the prevalence and pattern of serious physical violence in Chingola. Patients and Methods This was a prospective study. All patients who presented to Nchanga North Hospital and were admitted after violence were included in the study. Those patients who visited the hospital’s OPD as a result of violence but were not admitted were not included in the study. The study started in March 1999 and ended in March 2000. A detailed questionnaire was formulated and was filled in by the authors each time a victim of violence was admitted. Among the parameters studied were the age, sex, living conditions of the patients and injuries sustained. The victims were followed up in the wards from their day of admission to the day they were discharged. The injuries sustained were classified as minor injuries such as bruises small lacerations and muscle aches and major like large lacerations and head injury. The findings were analysed Results The number of patients admitted for violence related injuries over the one-year study period was 64; 44 were males and 20 females (M: F=2:1). There were 5000 admissions to the hospital during the year. The prevalence rate of injuries due to physical violence was 1.28%. The age ranged from eleven months to 62 years with a mean age of 30.1 years. Socioeconomic Factors Only 24 victims lived in houses with piped water and toilets inside the house; 20 lived in houses with piped water but with toilets located outside the house, the remaining 20 victims lived in houses without piped water and with toilets located outside the house. The victims who lived in homes with more than five persons were 40 (the average was 8 persons per home). Twenty four victims came from homes where there were less than five persons per home. The victims came from all the townships of Chingola with 61 victims coming from the medium and low cost areas (high density areas). Only 3 victims came from high cost i.e. low density areas. Seventeen females were assaulted at home; three were attacked outside the home. Table 3 shows the extent of alcohol consumption by the victims and perpetrators. History of alcohol consumption either by the victim or perpetrator was positive in 42 (65.2%) of the cases. All but 4 of the cases where the victim was the one who was drunk were cases of thievery. All the cases where the attacker was not known were for thievery reasons (Table 4). Fourteen women and 36 Male victims reported the matter to the Police but 6 males did not report. The weapons used in violence are shown in table 4. Only one case of gunshot was recorded. The injuries were classified as minor and major in 12 (60%) and 8 females (40%) respectively. In the males the minor and major injuries were equally distributed (50% each). Table 7 shows the degree of injuries according to the reason for the violence. Most domestic violence took place between 18.00 and 21.00 hours (Table 8). Hospital stay ranged from 1 day to 71 days with a mean stay of 6.6 days. Only one victim died (he was a male involved in a domestic conflict). Table 7. Reason of violence vs Severity of Injury.
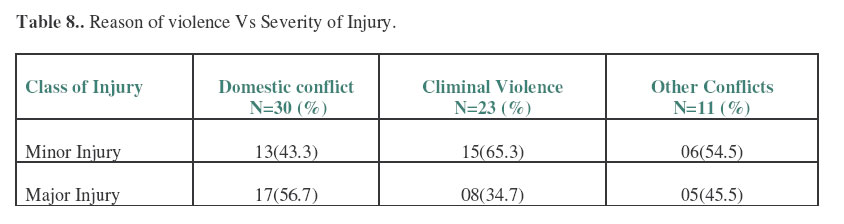
Table 8.. Reason of violence Vs Severity of Injury.
Table 9. Time of Violence.
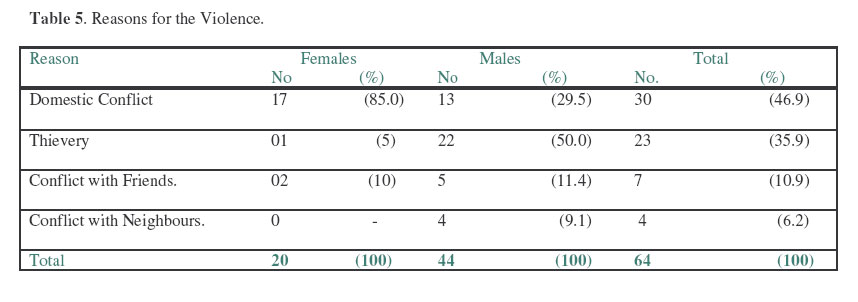
Discussion In one year of study there was a prevalence rate of 1.28% of admissions of people with significant violence related injuries. This prevalence ratio was similar to Peter Stuart’s in Australia although he looked only at Domestic violence1. In our study more men were victims of violence than women (M: F =2:1). This was similar to the findings of Patti Akers et all in Santiago5.In East England the largest age group among the intentional trauma victims was the 15 -24 age group2. Our most affected group was older-it is those who were aged between 21 and 30 years. This could be because they are the most active group socially. Wasiu et all found a similar age prevalence to ours in their study of maxillofacial injuries due to violence in Nigeria3,5 . The mean age for our patients was 30.1years. The obvious limitation of our study was that we concentrated only on those who got admitted. To get a truer picture we should have collected data from the Out patient department and the Police. The reasons for this were; we wanted to look at significant and not trivial physical assault, we also were skeptical about the record keeping of the other concerned departments. This is not only a problem here. Olasoji et all in Niger found that only 41% of the physical violence cases reported to the police were recorded7 When the living conditions of the victims were analyzed, it was found that 62.5% of the victims lived in less than acceptable situations in that they did not live in houses with piped water and water born toilets located inside the house. Similar percentages lived in homes with more than five persons per home (the average was 8 persons per home). These two factors suggest that the majority of the victims of violence came from the poorer section of the community. Even in Developed countries the strong association between socioeconomic deprivation and physical violence injury is well recognized e.g. the death rate due to injury in children from Social Class V is five times greater than that for children in Social Class I2,5 The violence was evenly distributed all the townships were represented but there were very few cases from Nchanga South town ship which is a low density/high cost area. Most of the victims were assaulted at home (53.1%). In fact all the females except three were assaulted at home. Alcohol was involved in 65.6% of the cases and in the majority of the cases it was the perpetrator of the violence who was under the influence of alcohol. There was a strong association between alcohol use and criminal activity in that all but four of the cases where the victim was the one who was drunk were cases of thievery. Thieves tended to take alcohol before they robbed their victims Peter Stuart in Australia showed in 2004 that the majority of the attackers in a domestic setting were husbands and ex-partners1 The most frequent known attackers in our study were the husbands followed by the neighbors and friends of the victim. However as expected, in cases of thievery the attacker was often not known. In total, domestic conflicts comprised 46.9% of the reason for the violence. However for women, domestic violence was responsible for 85.0% of the admissions. Reports show that Domestic violence is the leading cause of injury to women in the U.S and Canada6. This seems to support our findings. It is known that violence between partners in a relationship may be triggered by numerous factors, including stressful or frustrating life situations such as loss of a job, financial problems or pregnancy; role changes that may impact the attacker’s sense of control. Use of alcohol and/or drug abuse, which may increase abusive behaviour, is another common cause. Attitudes and traditional beliefs on the part of the aggressor that rationalize abuse are very common in Africa. Even sadistic personality of some aggressors may be the cause4. In this study we did not go into the actual causes of the conflicts at home. The next common reason for the violence was thievery. All the cases where the attacker was not known were for thievery reasons. In terms of timing, the most dangerous time for domestic violence was from 18 to 21 hours. Generally more than 50% of domestic violence occurred before 21 hours and most criminal violence from 21hours onwards. There seems to have been no particular date of the month most prone to violence. However there was a preponderance of violence occurring towards the month end and the beginning of the month. In more than 50% of the victims, fists, slaps and kicks were the means through which violence was inflicted. This was followed by acts of stoning and stabbing. The stabbing was done with knives and screw drivers. The use of the gun was not a feature in our findings. In other societies the picture of violence is quite different. Patti Akers et al in Santiago reported that firearm assaults were the leading cause of severe injury and death, followed by unarmed assault5 . Luckily, the gun culture has not yet gotten a hold in our society On analysis of the types of injuries, occasioned, it was found that more than half of the injuries were minor. However among the males 50% of the injuries were serious, and in the case females 40% of the injuries were serious. If one relates the reason for the violence with severity of the injury it comes out that the victim was more likely to get a serious injury in a domestic conflict than in criminal violence or other conflicts. All but six female victims (70.0%) reported the assault to the police, and among the male victims 36(81.8%) reported the matter. Olasoji et all7 in Niger found a much lower percentage (58%) of reporting to the police, the main reason given by those who did not report being that they thought nothing would come out of it7. In our case, the variance in reporting was because women were mainly assaulted at home and were most likely intimidated by their attackers, so they did not report. On average these patients stayed six days in hospital, but most patients stayed four days. There was one death recorded; this was that of a male victim involved in a domestic conflict. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07013t7.jpg] [js07013t1.jpg] [js07013t6.jpg] [js07013t8.jpg] [js07013t9.jpg] [js07013t4.jpg] [js07013t5.jpg] [js07013t2.jpg] [js07013t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}