 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
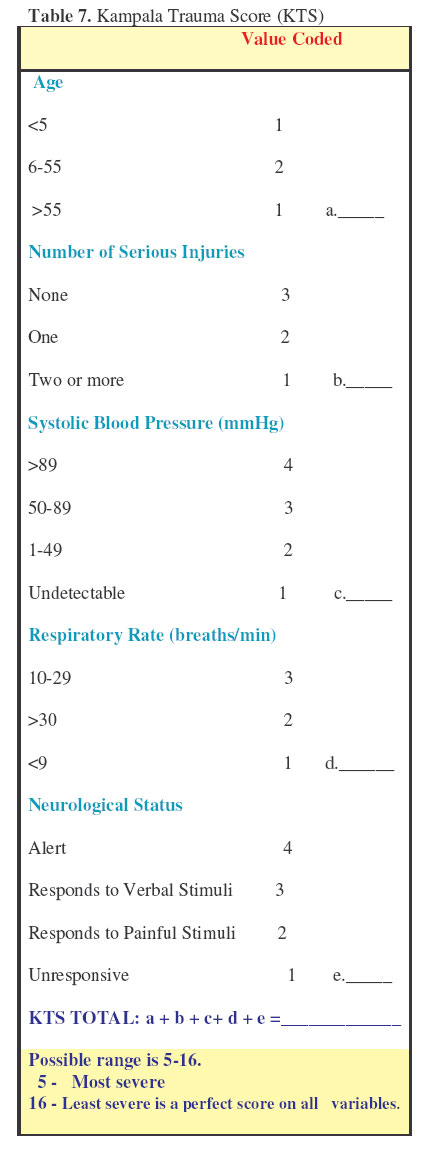
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 74-82 Kampala Trauma Score (KTS): Is it a New Triage Tool? Macleod1 ,J.B.A.; Kobusingye2, O.; Frost3, C. & Lett2,4, R. 1Department of Surgery, Emory School of Medicine, Atlanta, USA, Code Number: js07014 IntroductionIn North America, injury surveillance has generated an accumulation of data regarding trauma events and outcomes through the implementation of trauma registries. Trauma registries have been predominantly instituted in response to the desire to be accredited by the American College of Surgeons (ACS). Committee on Trauma as an ACS Trauma Center1. These registries play a key role in research that determines epidemiological patterns of injury, advances injury prevention actions and finally, measures outcomes2. For example, they have been used extensively in the US to monitor reductions in mortality which has been attributed to the institution of “trauma systems”, coordinated hospital-based systems for the management of injured patients3. As interventions to reduce and prevent injuries are sought, registries allow the calculation of injury rates, identification of causes and measurement of outcomes produced by implementation of interventions4. Trauma registry data is made universally comparable across different strata through the routine use of trauma scores, such as the revised trauma score (RTS) and injury severity score (ISS). To facilitate injury surveillance, injuries have been coded by severity instruments which grade the severity of an injury. This enables the comparison of injuries despite their diversity. Numerous scores have been advocated and to date, there is no one score in the literature which has emerged as the gold standard5. These scores can provide the basis for policy development in the area of human and other resource allocation and also allow institutional quality assurance2 . These injury scores have lead to normative standards which permit inter-institutional comparisons in industrialized countries. Outside these research functions, it has been hypothesized that severity scores could also potentially function as triage tools. In 1996, a trauma registry was introduced in Kampala, Uganda at Mulago Hospital through the supervision of the Uganda Injury Control Center (ICC-U). A new severity score, Kampala Trauma Score (KTS), was developed. This is a simplified composite of the Revised Trauma Score (RTS) and the Injury Severity Score (ISS). The KTS has been validated for its ability to predict outcome in the Ugandan trauma registry6 . The KTS has been shown to perform comparably to the RTS and ISS when evaluated statistically7. In this last study, the KTS was also assessed for its potential as a triage tool but on only a small cohort of severely injured patients (ISS> 16). However, the function of the KTS as a triage tool when used with a cohort of all injured patients presenting to a health care facility within a resource constrained environment has not been reported. Thus, the aim of this study was to evaluate the potential usefulness of the KTS to differentiate injured p patients at high risk for a poor outcome as opposed to those who were unlikely to have a poor outcome at the time of their presentation to a health care facility. We hypothesized that the KTS could be used as a triage tool for health care personnel to determine decision-making regarding individual injured patient’s needs even if applied to all injury patients presenting at health care facilities for assessment and treatment. This would assist the appropriate referral and treatment of patients and reduce morbidity and mortality while minimizing unnecessary cost and expenditure. Methods The data from November 1, 1996 to May 31, 1999 collected by the Ugandan Trauma Registry from two hospitals, Mulago in Kampala and Kawolo in Mukono, were reviewed. All patients entered in the database who were 16 years of age and older were included. All data was collected by the casualty staff manually on a standard collection sheet and was entered into an Epi-info database by a single ICC-U staff member. The KTS was calculated by the casualty personnel and entered as recorded from the form as an ordinal scale variable. Calculation by the ICC-U staff was done, if the KTS was not entered on the form but all necessary information on the form was filled in. Descriptive statistics were performed utilizing all the variables except for the geographical information. Age was recoded into a categorical variable with five year age bands up to age 30 then one ten year age band from 31-40 and the last age band for all those 41 and older. This categorization best reflected the age distribution. KTS and age had skewed distributions and therefore, were described with the median and range. The distribution of the possible range of KTS scores was analyzed for two outcomes: the occurrence of death at 2 weeks and the need for admission. The outcome in the casualty ward was recorded by the attending medical personnel as “treated and sent home”, “admitted” or “ died”. The medical records department at two weeks completed the outcome of the patient’s injury, as “died”, “discharged” or “ still in hospital” irrespective of the exact timing of the event during the two weeks. The injury score, KTS was evaluated over all possible cut-off points. The 95% CIs, for the sensitivity and specificity, were calculated from the binomial distribution. For this analysis, the outcomes were recoded as binary in the following manner:
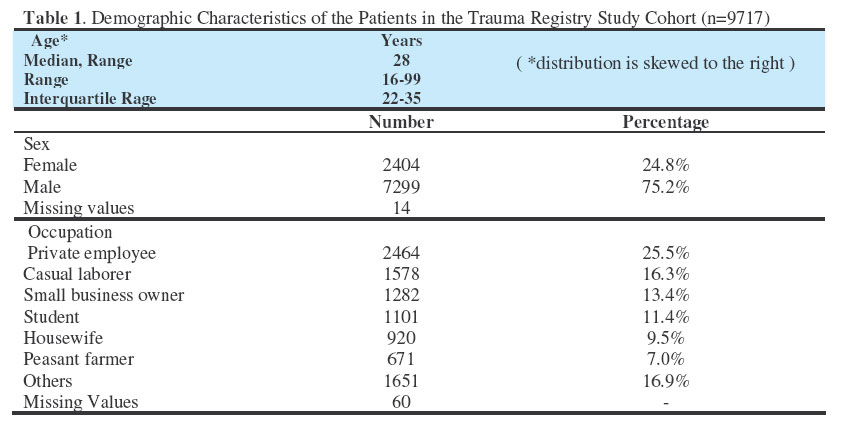
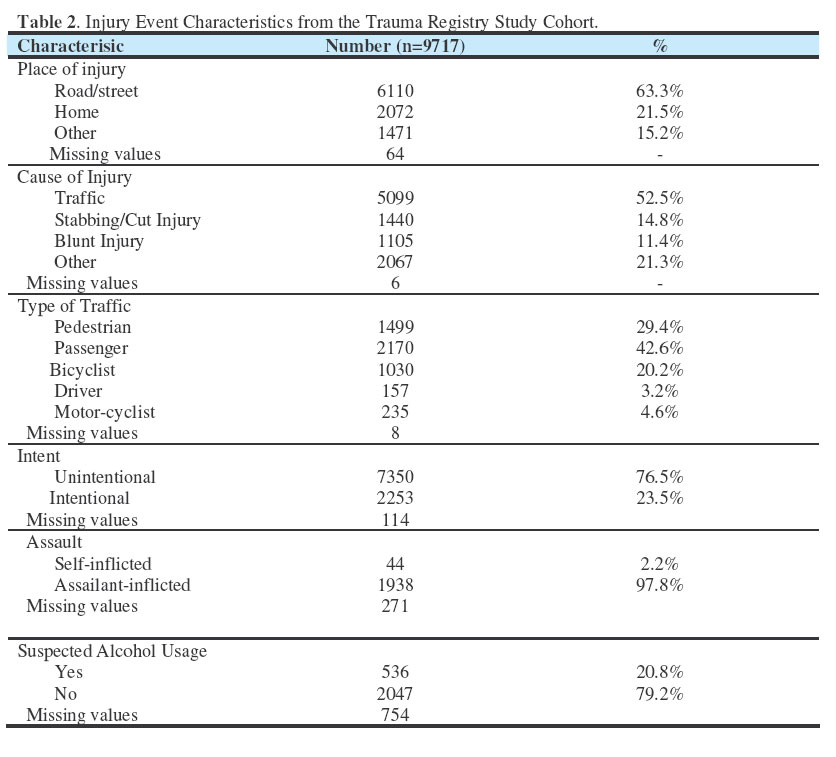
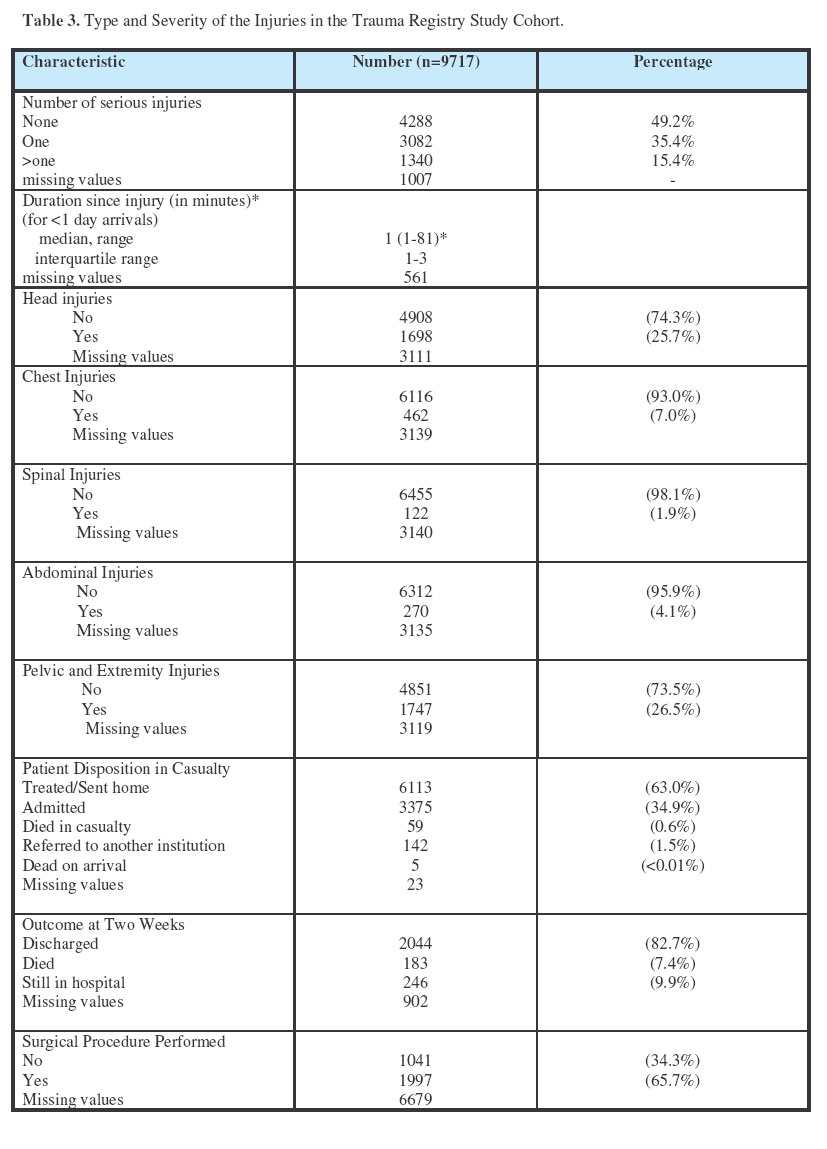
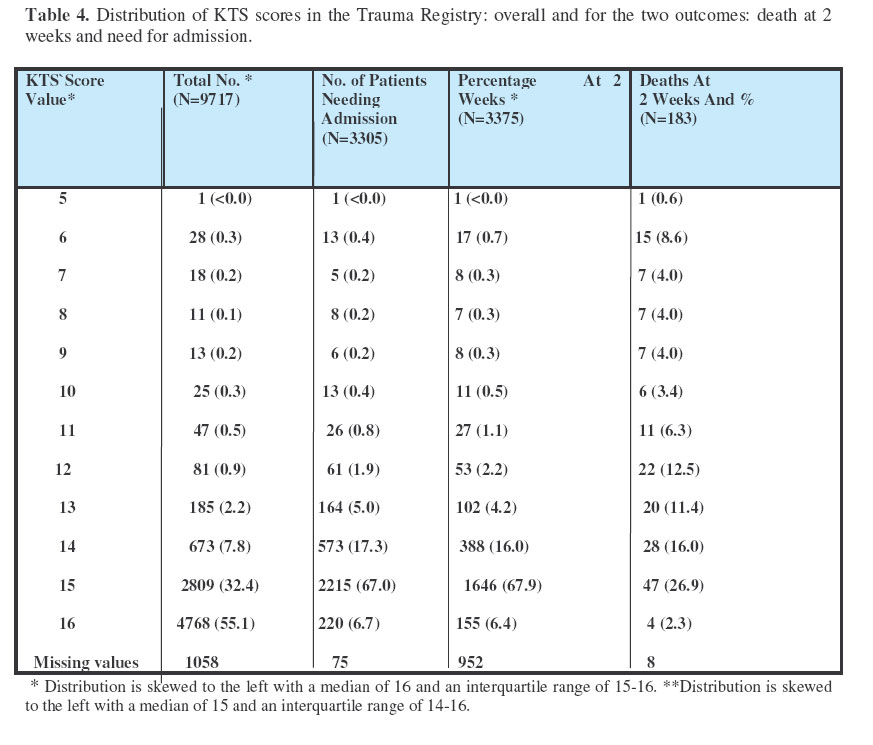
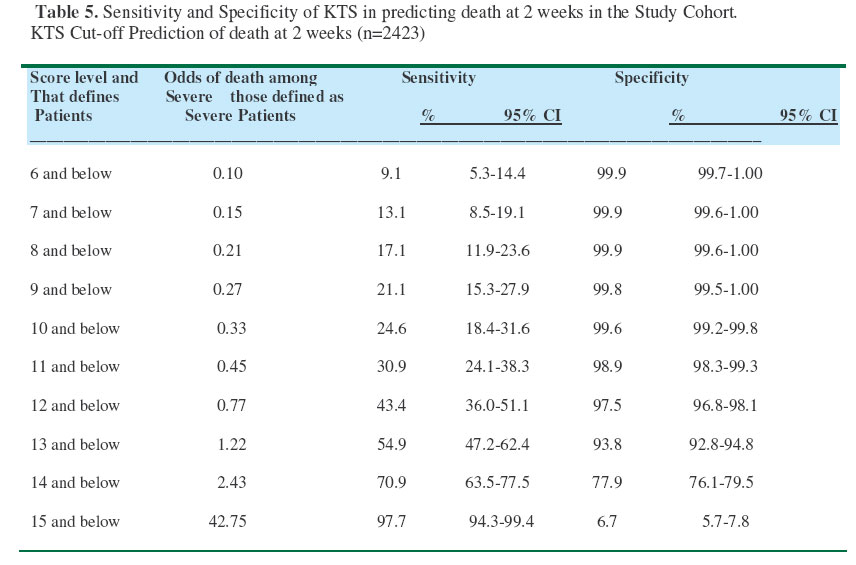
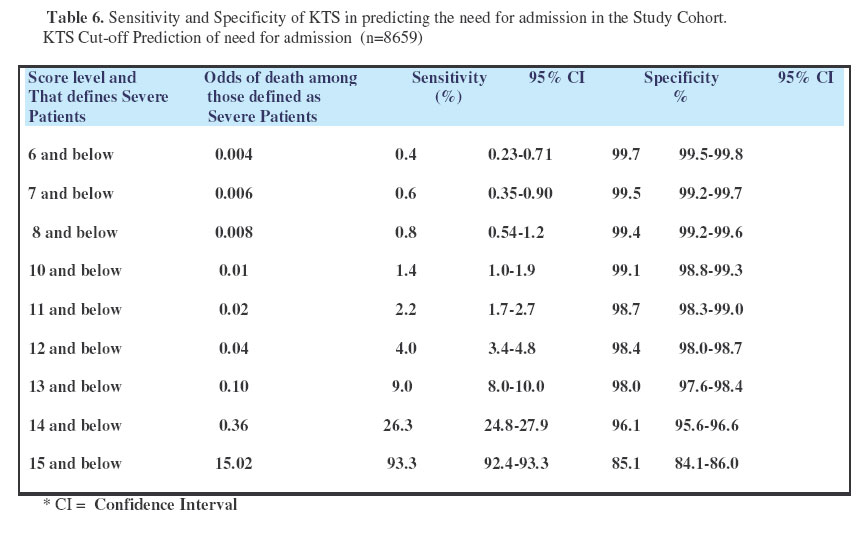
The software packages, Epi-info 6.0 and Stata 6.0, were used for all data analysis. ResultsThere were 9,777 patients in the Trauma Registry during the study period and 9,717 had data available for evaluation. Table 1 shows the demographic characteristics of the study cohort. Approximately half of the injuries occurred in patients between the ages of 22-35 with a median age of 28. Three-quarters of the injuries occurred in males and the age distribution was similar for both genders with medians of 28 and 27, males and females respectively. Employees and casual laborers were more represented than peasant farmers. The injury events characteristics are summarized in Table 2. Three-quarters of the injuries were from road traffic crashes. Of these crashes, the injured person was most frequently the passenger, followed by pedestrians. Assailant-inflicted stabbing was the second most common cause, recorded in 14.8% of the patients. Since 1998, the recording of alcohol consumption by clinical judgment has shown that 23.9% of the patients had consumed alcohol. However, under-or over-reporting depending on the medical personnel’s bias is likely as no blood alcohol examination was performed. Table 3 shows that 49% of the patients recorded in the injury registry had no serious injury. There were 59 (0.6%) deaths in the casualty and 183 (7.3%) deaths occurring within two weeks among those admitted. The median duration from injury was one day. For those who arrived on the same day, the median time to arrival was 11/2 hours. There were 1,997 surgical procedures performed in total but only 640 of these were performed on individuals who were admitted. Therefore, surgical procedures even of a minor nature from which patients could be later discharged, were included. There was a wide range of missing values for all variables (except for age), that ranged from 6 for “cause of injury” to 6,679 for “surgical procedure performed”. The KTS in the surveillance database ranges from all the possible scores, 5-16. The most commonly reported score was 16, a perfect score on the KTS: normal physiologic parameters, age between 5-50 and no serious injuries (Table 4). The distribution is severely skewed to the left with the two highest scores, 15 and 16 representing 87.5% of all the records. Table 4 shows the distribution of the KTS among all patients as well as among the patients with outcome information available who were included in the analyses. For those patients whose outcome most needs to be predicted, and therefore whose triage is most crucial, those who were admitted or died as assessed by our study’s outcome indicators, the KTS score of 15 showed the highest frequency of occurrence. Triage utilizes numerical cut-off points along the score’s continuum to predict the greatest number of people who would have a poor outcome, “severe” patients, when scoring below the threshold and a good outcome, “non severe” patients, when scoring above the cut-off or numerical threshold. In our study, outcomes of interest to predict were death versus survival and continuing hospitalization at 2 weeks versus discharge. In Tables 5 and 6, the sensitivity and specificity of the KTS to predict death and need for admission at all the different possible cut-offs that could be used for triage decision-making is shown. The odds of death at 2 weeks or of need for admission increase as the KTS cut-off increases. Sensitivities are low until one reaches a high value for the cut-off of 14, but at a significant loss in specificity dropping from 94% to 78% (Table 5). This cut-off would still identify 74% who were above 14 (Table 4). However, with the outcome being death, the sensitivity of only 71% means that 29% of those who die would be scored as non-severe. It should be noted that the specificity drops to 6.7% at a cut-off of 15 due to the nonrandom loss of a high proportion of patients who scored 16 and were discharged with no outcome data available. Need for admission among those who truly need admitting, is only detected when the numerical cut-off used for severe versus non-severe is 15 and below. At this point, the sensitivity is 93% and the specificity is 85% (Table 6) Table 4. Distribution of KTS scores in the Trauma Registry: overall and for the two outcomes: death at 2 weeks and need for admission.
* Distribution is skewed to the left with a median of 16 and an interquartile range of 15-16. **Distribution is skewed to the left with a median of 15 and an interquartile range of 14-16.
However, the definition of a serious injury for the KTS, as is outlined in the Trauma operative guidelines (produced by ICC for use with the injury surveillance registry), includes an injury “considered serious enough to warrant admission on its own merit”. Therefore, even if a patient can be scored for several reasons as a 15, in certain cases it can be associated with admission purely by definition. At the cut-offs below 15, the sensitivity for predicting need for admission is 26% or lower. The performance of the KTS (Table 7) in predicting these two separate outcomes can not be directly compared because the analysis is based on two different groups of patients Table 4). The group in whom “death at two weeks” was analyzed is a nonrandom subset of the group analyzed for “need for admission”. In conclusion, the KTS in the injury registry database is not a very sensitive score but has a reasonable specificity. DiscussionAn injury surveillance registry can be very useful for descriptive data in regards to patterns and causes of injury. From this database, it can be seen that the pattern of injuries is similar to what has been described in the literature for industrialized countries8. Road traffic injuries are the leading cause of injury as is seen in most countries world-wide, males are more commonly involved with a skew of the age distribution towards the under 35-years old adults9. The overall mortality rate was 7.3% which is consistent with but slightly lower than has been previously reported in the literature10 . This difference may be explained on the basis of the trauma registry being hospital-based, while community surveys show that in resource-poor settings the majority of deaths occur prior to arrival at hospital11 . This trauma registry has a high proportion of “mildly injured” patients, over fifty percent scored a perfect score of 16 on the KTS, 65% were treated and sent home and less than half had no serious injuries. All injured patients who presented at the health care facility and who survived to admission but died within two weeks are included but no information about deaths prior or after the 2 week period is available. Therefore, the limitations of the predictive capability of the KTS for mortality from this registry data may be a reflection of the characteristics of the study cohort and may reflect a reduced predictive power of triage by KTS in mildly injured as opposed to severely injured patients. In a cohort of 150 trauma patients at Mulago hospital, a higher incidence of death was found in comparison to the probability of death predicted by the TRISS score.13 Therefore, issues such as a lack of equipment and manpower resources also could contribute to appropriate and timely care for the injured in resource constraint environments, resulting in an increased incidence of death. These multi-factorial causes of death, often seen in the African context, could impact the ability of death within the first 2 weeks to be predicted by a score taken only at admission. A score, such as the KTS, follows the Western-utilized scores of RTS, ISS or TRISS where system issues such as physical, equipment and personnel resources are not accounted for in the scoring instrument’s prediction of survival. This is a possible contributing factor to the limited predictive capability of the KTS. This study is limited by the possible selection bias seen in the cohort. The Uganda Injury Surveillance Registry is well supervised, now firmly entrenched in the casualty ward routine and one of the few if only ongoing injury surveillance systems in Africa. However, there were a large number of incomplete records, with age being the only completed variable in all records examined. The variables assessing injury type, severity and outcome were the least complete, with missing rates of up to 35%. This reduced sample size and affected the statistical power of the analysis. This incomplete enrollment also introduces bias with a selection toward the less severe cases, 87% of the patients scored either a 15 or 16 on the KTS. Are 87% of the patients entered into the registry as 15 or 16 because they are being labeled incorrectly by the KTS? This study has shown that the sensitivity of the KTS is low with a reasonable specificity. Of the total deaths, 47/183 or 26% of them occurred in patients who were given a KTS score of 15. There were 4 patients who received a perfect KTS score of 16 but went on to die within the two week period. Would the KTS perform better on a more select subset of patients as opposed to a surveillance registry that includes all trauma admissions? The KTS score is a severity instrument designed to differentiate severe injuries from non-severe injuries. However, the outcomes it predicts, mortality and prolonged hospitalization, are often not as frequently involved and vary less widely for non-severe injuries. Also, the relationship between these patient outcomes and injury severity is neither linear not binary in its nature, making the use of cut-offs difficult.12 If the KTS score categorizes patients as “severe”, a more effective application of clinical interventions, can be applied to those who will gain the most. In the trauma registry, at its “best cut-off” (70.9% sensitivity, 77.9% specificity) the KTS will still mislabel 29% of the patients who will go on to die. Therefore, the KTS is more difficult to utilize for individual patient triage as opposed to its potential usage to determine for example, resource allocation on a population-wide basis. Therefore, this study was unable to determine a cut-off point for differentiating severe versus non severe patient populations that would allow targeting of health interventions on an individual basis as may be used by health care personnel. Until further applied research is undertaken, the KTS’s usefulness as a triage tool is limited. However, it will continue to be used effectively for population-based approaches to health care needs assessment, evaluations and research. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07014t5.jpg] [js07014t1.jpg] [js07014t3.jpg] [js07014t6.jpg] [js07014t2.jpg] [js07014t7.jpg] [js07014t4.jpg] | ||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}