 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
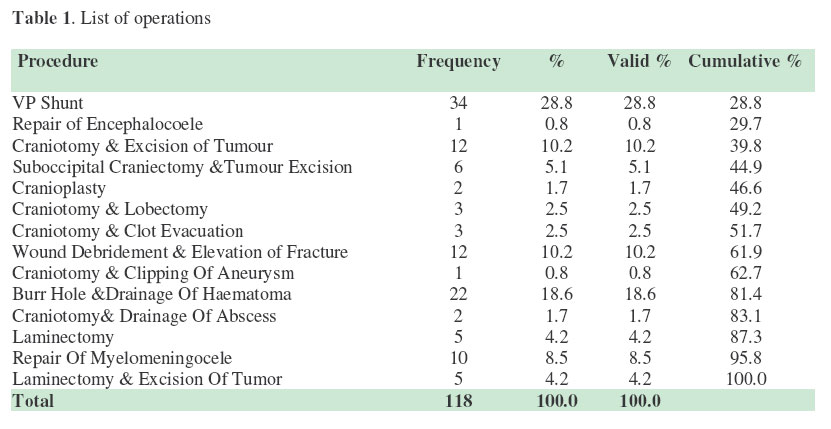
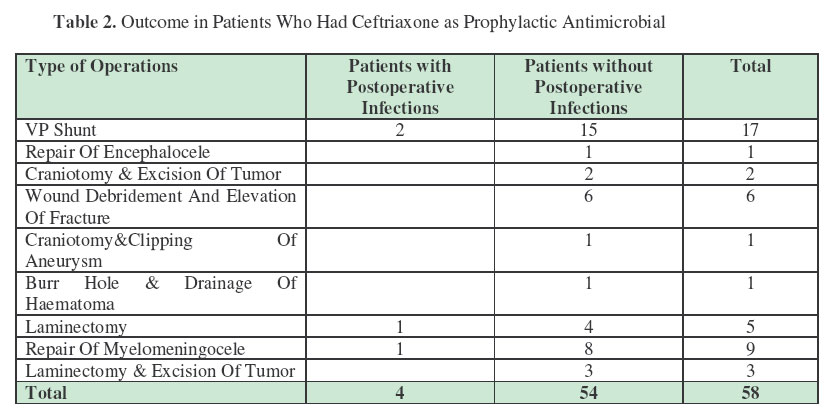
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 89-92 Prospective Comparative Trial of Ceftriaxone versus Ceftazidime as Prophylactic Perioperative Antimicrobials in Neurosurgery Malomo, A.O.; Adeolu, A.A.; Odebode, T.O.; Komolafe, E.O.& Shokunbi, M.T. Department of Neurological Surgery -UCH, Ibadan Code Number: js07016 Background: Previous reports have suggested that both ceftriaxone and ceftazidime are effective as prophylactic perioperative antibiotics in neurosurgery. This study was designed to compare the infection rates following the use of these antibiotics as prophylactic agents during neurological surgery in our centre. In a tertiary hospital Introduction Ceftriaxone and ceftazidime are both potent antibiotics belonging to the third generation of cephalosporins. They have broad spectrum activities against gram-positive and gramnegative microbes. Although the choice of prophylactic antibiotics for neurosurgical procedures is not fully established as several regimen have been used1-6 , the morbidity and mortality that often accompanies postoperative intracranial infections have compelled us to consider these antimicrobials as prophylactic antibiotics in our centre. In addition, we have observed higher infection rate in other previously used antimicrobial agents. Previous reports have also demonstrated the use of these agents in neurosurgical operations7-10 . In this study we compared the infection rates in our patients who received either ceftriaxone or ceftazidime as prophylactic perioperative antibiotics. Patients and Method This prospective study was carried out between September 1998 and December 1999. Consecutive patients were allotted into two groups; Group I received intravenous ceftriaxone (Roche - Rocephine) 100mg/kg daily for two days while Group II received intravenous ceftazidime (GlaxoSmithKline – fortum) 50mg/kg every twelve hours for two days. The first dose of antibiotics was given at induction of anaesthesia. We also used irrigation fluid containing 40mg of Gentamycin in 500 ml of normal saline in all the patients. Patients who had evidence of intracranial or scalp infection and those on antibiotics before surgery, were excluded from the study. Clinical and/or laboratory evidence of wound infection or intracranial infection was used as outcome measures. The patients were followed up in the ward and in the clinic for six weeks. We analyzed the presence or absence of wound infection, demographic data, diagnosis and type of surgical procedure. The statistical significance of the difference in infection rates in the two groups was determined by Chi-square. The pvalue less 0.05 or less was considered as significant. Results There were a total of one hundred and eighteen patients. Fifty eight patients received ceftriaxone and sixty patients received ceftazidime. The age range was 1 month to 94 years with a mean age of 24.86. Table 1 shows the various procedures performed during the study period. Ventriculoperitoneal (VP) shunt for hydrocephalus was the most common procedure performed with a frequency of 38 (28.8%). Only 1 patient had craniotomy and clipping of aneurysm. Table 2 shows procedures in which ceftriaxone were used in the irrigation fluid. VP shunt for hydrocephalus was the most common procedure followed by burr hole drainage of subacute and chronic subdural haematoma. Infection occurred in four procedures in this group. Two out of these were in the patients who had VP shunt. The overall infection rate was 6.9%. The infection rate in VP shunt procedures was 11.8%. Table 3 shows the procedure in which ceftazidime was used. The pattern is similar to table 2 with VP shunt for hydrocephalus being the most common procedure followed by burr hole drainage of subacute and chronic subdural haematoma. Nine patients had infection with infection rate of 15%. Two of the 17 patients who had VP shunts had infection as in the ceftazidime group. The infection rate in VP shunt procedure was similar to the infection rate in ceftriaxone group. Table 3. Outcome in Patients Who Had Ceftaziime as Prophylactic Antimicrobial
Table 4. Relationship between Patients with and Without Postoperative Infections in the Two Groups.
X2 = 1.975, df 1; p=0.160 There were 9 patients with infection in ceftazidime group compared to 4 patients in the ceftriaxone group but this was not found to be statistically significant (Table 4). DiscussionThe study was carried out in a wide range of neurosurgical procedures. The infection rates are quite high compare to infection rate reported from other parts of the world1,2,4,5,6,11,12 . This may be related to many factors including poor patients’ personal hygiene and inadequate sterilization of the instruments, theatre gown and drapes due to imperfect sterilization techniques. These are peculiar problems of the developing world. Improvement of these various factors will certainly help to improve the infection rate in our neurosurgical procedures. Surprisingly, the infection rate following our VP shunt procedure is comparable to reports from other parts of the world13. This may be related to the short duration of follow up in our series or perhaps because of the greater attention to meticulous aseptic techniques during VP shunt procedure. The overall infection rate was higher in ceftazidime group (15%) compared to ceftriaxone group (6.9%). This difference was, however, not statistically significantly. Furthermore, the infection rate in VP shunt procedure was the same in both groups with a value of 11.8%. This result is not surprising because both drugs are third generation cephalosporin with similar mechanisms of action. Their spectrum of activity is also fairly the same. In addition, the two antimicrobials have been found to be effective as prophylactic agents in neurosurgical procedures1,3, 7-11, 14-16 . The total cost for our regime for ceftriaxone is
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07016t2.jpg] [js07016t3.jpg] [js07016t4.jpg] [js07016t1.jpg] |
| |||||||||

{kind=link}
{kind=link}