 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Gross Anatomical Variations and Congenital Anomalies of Surgical Importance in Hepatobiliary Surgery in Uganda.Ibingira, C.B.R. : Senior Lecturer and Head of Department of Anatomy Faculty of Medicine Makerere University. P.O. Box 7072 KAMPALA.Email : cibingira@yahoo.com. Code Number:js07017 Background: It is important for surgeons to appreciate the possible anatomical variations that can be encountered during surgery. This study was aimed at determining the gross anatomical variations and congenital anomalies of the external hepatobilliary system in Ugandan cadavers and to describe the nature and contents of the gallbladder among cadavers of Ugandans. Introduction The extra hepatic biliary system is composed of the:
Anatomical Location The liver and Gall bladder are located in the abdomen, the bulk of the liver lies in the right hypochondrium, epigastrium and left hypochondrium. It has two surfaces:, the diaphragmatic and visceral. The gallbladder lies in the right hypochondrium, in a shallow fossa on the quadrate lobe of the liver, with its fundus touching the anterior abdominal wall at the point where the tip of the ninth costal cartilage meets linear semilunaris, its continuous with the body and the neck that narrows into the cystic duct. Usually the gallbladder lies to the right of the porta hepatis. The fundus is completely peritonized while the body and neck are only peritonized on three sides1,2 . The porta hepatis is one of the bare areas of the liver, as well as the gate way into and out of the liver apart from going through or out of the other bare areas of the liver which are located in the following sites 1. Gall bladder fossa
The structures that come out are:
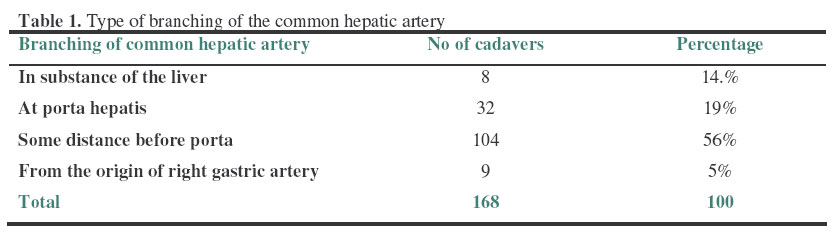
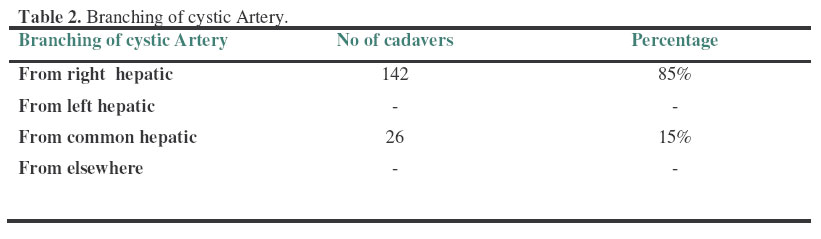
Other parts of the hepatobilliary system on the visceral surface include; the common hepatic duct, hepatic artery and portal vein. The common hepatic duct is joined by the cystic duct to form the common bile duct. The distance at which they unite is quite variable3,5,6,7 but the average length is 8-10 cm6 , it runs down to open at the posteromedial aspect of the second part of the duodenum. It lies within the gastro hepatic ligament (lesser omentum) to the right of the common hepatic artery and anterior to the hepatic portal vein, all the three structures lie anterior to the epiploic foramen of Winslow6,7 . The cystic artery usually branches from the right hepatic artery, and passes behind the common hepatic duct to reach the gallbladder3,6,7. In 15% of the cases the right hepatic artery and or the cystic artery cross in front of the common hepatic duct. The common hepatic artery originates from the celiac trunk, runs to the right posterior to the lesser omentum to reach the superior part of the duodenum where it gives off the gastroduodenal artery and ascends to the liver. ,.usually it may give off the right gastric artery before it divides into the two terminal branches, but variations of the course of this artery are common3,6,7 . The most dangerous anomaly and or variation is when the hepatic artery takes a tortuous course anterior to the origin of the cystic duct with a very short cystic duct6. Other congenital anomalies of the hepatobilliary system may include; absence or floating of the gallbladder, doubling of the gallbladder ,absence of the cystic duct, a low or high insertion of the cystic duct, low insertion where it opens close to the ampulla while in a high one it joins the common hepatic duct close to the liver3,5,6,7 . Open or laparoscopic cholecystectomy, orthoptic liver transplant for liver tumours, gastric or any other hepatobilliary surgery, are among the most frequently performed operation in the upper abdomen. The described relationship of the gallbladder, cystic ducts, hepatic ducts, the bile ducts, associated blood vessels is what is generally known and expected when performing any of those operations. It should be noted however that considerable anatomical variations may exist in a given population and knowledge of such anomalies is of utmost importance to the surgeon, because failure to recognize them at operation may lead to a disaster. Severing of an anomalous or accessory hepatic duct without ligature of its cut end, would result into biliary peritonitis while at the same time mistaken ligature of an abnormally placed right hepatic artery might be fatal. Other anomalies may render the right hepatic duct or common bile duct or any of the arteries liable to injury5,6,7,89,10,11,12,13,14 . Most errors in gall bladder surgery result from failure to appreciate the common variations in the anatomy of the biliary system5. The success and safety of laparoscopic cholecystectomy, orthotopic liver transplantation, and trisegmentectomy for hepatic tumors and any surgery on the hepatobilliary system depend on a high regard for and an accurate knowledge of the anatomy and some of the common embryologic anomalies of the biliary tree. The blood supply, ductal variations, and gallbladder anatomy of this area are often the source of major challenge to unprepared and unaware surgeons. There should be a great attempt to stimulate an interest in, a respect for, and perhaps a lot of desire to learn more about the important and fascinating anatomy of this region12,13,14 . This study was aimed at determining the anatomical variations and anomalies in the extrahepatic billiary system among Ugandan cadavers. MethodsThis was a cross sectional study done in the gross anatomy dissection laboratory of Makerere Medical School on cadavers for a period of eight years between October 1997 to June 2005. All the 21 cadavers dissected each year were recruited into the study each year for 8 consecutive years, but were first examined to note the sex. This was followed by an excellent dissection to display the gross anatomy of the visceral surface of the hepatobilliary system noting the following parameters.
Results Table 3. Distance of branching of the cystic duct from the opening of the common bile duct.
Table 4: Length of the common bile duct
A total of 168 adult cadavers were involved in the study; of which 56 were females and 112 were males. The male to female ratio was 3:1. In 160 (95%) of the 168 cases, the common hepatic artery originated from the coeliac trunk, while in 8 (5%), the origin was the superior mesenteric artery. The cystic artery was found to originate from the right hepatic artery in 142 (85%) of the cases while in 26 (15%), it came from the common hepatic artery. In 104 specimens the course of cystic artery was anterior to the right hepatic duct and it passed posterior to right hepatic duct in 38 of the cases. It traveled posterior to common bile duct in 2 cases where it originated from the common hepatic artery and in this case there was more than one cystic artery – others being very small and branching from high up. In 26 of the cases it passed anterior to the common bile duct to reach the gall bladder. It was noted that the commonest branching was within 2-6cm before the porta hepatis to form right and left hepatic arteries. It was also noted that the level of branching affected the source of the cystic artery; a lower branching at level of gastric artery, resulted into there being more than one cystic arteries and division of the artery into the substance of the liver was associated with a varied source of the cystic artery., and in this study the cystic artery originated from common hepatic artery in 28 cadavers. In 97.6% the cystic duct branched off from the common hepatic duct. In one case however, the cystic duct joined a smaller accessory billiary duct (Table 3). A total of 67% of the ducts had low branching, indicating that the length of the common bile duct was shorter than in high branchingThe mode was 4cm in length meaning that in this study the majority of cadavers had a short CBD, the average length being 5.1cm, and more than 50% falling below half the measured lengths indicating that low branching is very common. Presence of Gallstones.Although it was not part of this study, it is worthwhile noting that gallstones were found in 7 (5%) of the cadavers. DiscussionIn this study the male to female ratio was 3:1. The previous studies however, did not indicate the gender distribution3,4,5,6,7,8 . The majority of the cadavers were average weight and this could in part explain why the number of cases of gallstones was low since it is generally known that that gallstones are prevalent in the fat people1,2 . In only 5% of cases did the hepatic artery originate from the superior mesenteric artery in this study. This finding was a significantly variation from other reports where the incidence was found to be 12%3,6,7, though the course of the artery and its relations with the common bile duct (CBD)and the hepatic portal vein were almost constant. Therefore during abdominal surgery, especially on the pancreas, care must be taken not to damage the hepatic artery when it arises from the superior mesenteric artery. In 85% of the cases studied, the cystic artery originated from the right hepatic artery. Similar findings have been reported from other populations3,5,6,7 . The next most frequent origin was from the common hepatic artery. None of the cases in the present series had its cystic artery source from other neighbouring arteries such as the gastroduodenal, pancreaticoduodenal, right gastric, left hepatic and superior mesenteric arteries which had been observed in other studies5,6,7 . It has been noted that the vessels that give off the cystic artery are those that are closest to the gallbladder3,6,7 . Several bodies had more than one big cystic artery, and the small accessory artery. This is a very common finding in other populations especially where the branching of the common hepatic artery is varied3,6,7,8 . Since the source of the cystic artery is varied, it is better to follow it retrograde from the gallbladder to its source, this is particularly important when there are accessory cystic arteries to ensure proper artery ligation during surgery. in such circumstances however, the safest ligation is one closest to the gall bladder, because near the origin of the cystic artery, there are many vital structures that could be damaged since there may be variations. The course of the cystic artery was found to be varied in 61% of the cases. The artery crossed anterior to the right hepatic duct, and in28% of the cases it passes posterior to the right hepatic duct. This is different from what was reported in other studies where only in 5% it passed posterior to the right hepatic duct6,7 . For those arteries passing anterior, there are many variations brought about by the source of the cystic artery. For instance, 13% of arteries arose from a low lying right hepatic artery and 2.1% and 2.6% arose from the common hepatic artery and right gastric artery respectively. In this study, in 5% of the cases it passed posterior to the CBD, and in 10% it passed anterior to CBD.The course and origin of this artery are of utmost importance in gallbladder surgery. Its association with the right hepatic duct, CBD, left hepatic duct, and the underlying hepatic portal vein puts all these structures at a big risk and may result into un rectifiable or fetal complications, if such pertinent variations are not in the surgeons memory. The level of branching of this artery should be born in mind because it is the one that determines the origin and course of the cystic artery 2,6 . Looking at the branching of the cystic duct in this study, its only in 2% of the cases that the cystic duct joins or branches from the right hepatic duct, however irregular branching of the cystic duct has been reported to being common in other studies3,7,810,11,12,13,14. In some cases the cystic duct opens into an accessory hepatic duct rather than joining the common hepatic duct to form the common bile duct, this only occurred in 0.6% of the cases in this study. In this study, the types of junction of the cystic duct with any of the hepatic ducts were not considered, however in other studies, this variation was considered whereby an acute angled junction occurred in 67% of the cases, the short parallel junction type came second and the posterior junction with a spiral course occurred least. The level of branching of the cystic duct in this study was predominantly low ,and this contributed to the shortness of the CBD ,where the most frequent length was 4 cm, the lowest being 2.5cm and maximum being 12cm. This shows that the CBD is very short as compared with other studies where the mode was 8-10 cm7. No anomalies of the gallbladder were found in this study, unlike other studies3,5,6,710,1112,13,14 . Conclusion.From this study, it can be concluded that:
To avoid errors, complications, and disasters during hepatobiliary surgery, The surgeons need to appreciate, and to have knowledge of the common Anatomical variations of the hepatobilliary system in a given population. As for any hepatobiliary procedure, awareness of possible anatomical variations of the extrahepatic biliary system, intraoperative identification of the anomalous ducts, vessels and appropriate tailoring of the surgical technique are advisable in order to avoid serious postoperative complications.. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07017t3.jpg] [js07017t2.jpg] [js07017t4.jpg] [js07017t1.jpg] |
| |||||||||

{kind=link}
{kind=link}