 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
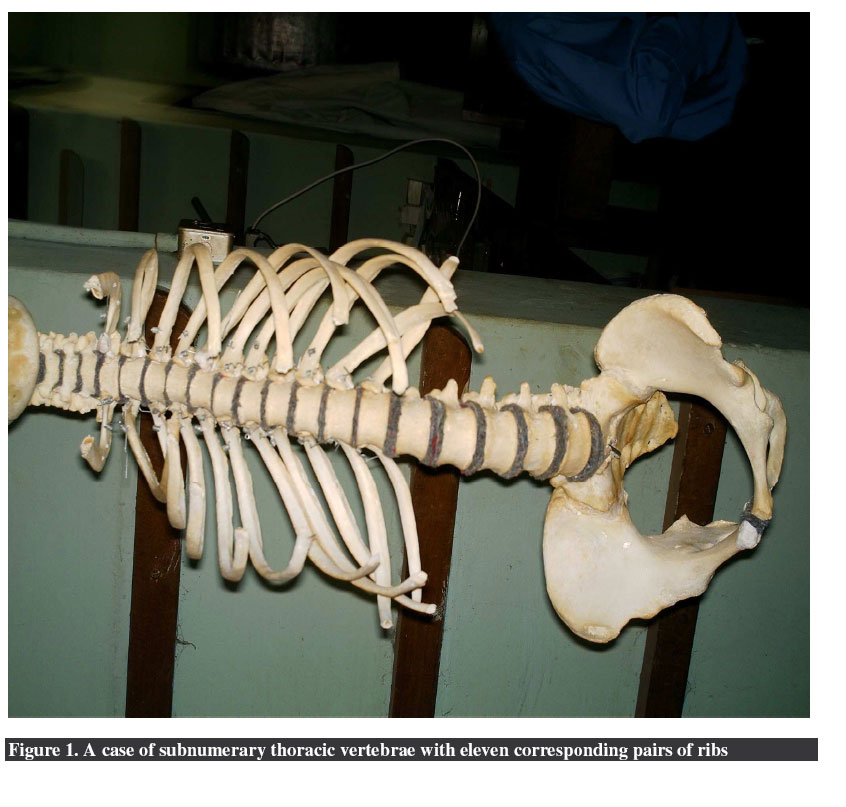
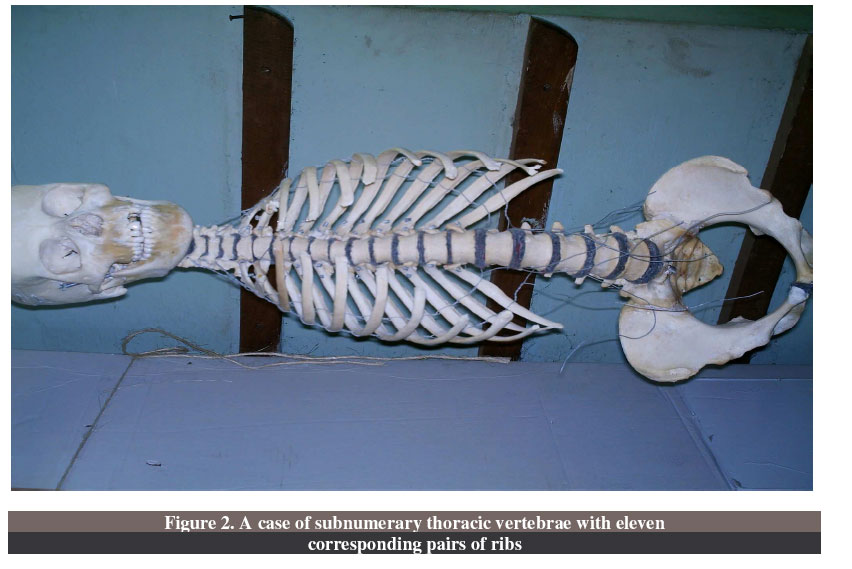
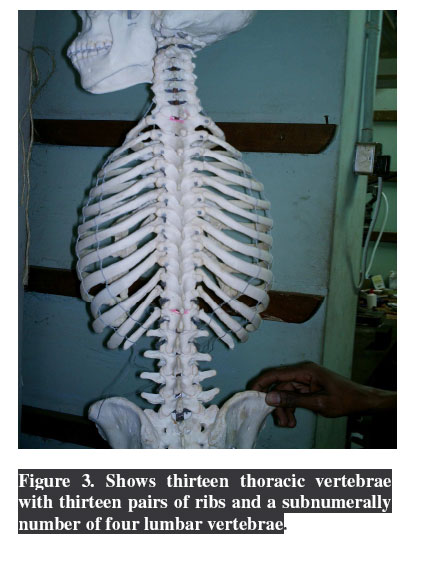
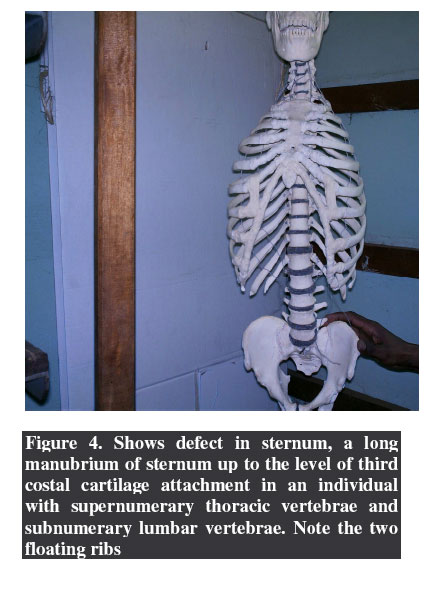
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 99-104 Sternal Anomalies with Supernumerary and Subnumerary Vertebrae and Ribs – Case Reports Ochieng, J. & Ibingira, C.B.R. Department of Anatomy, faculty of medicine, Makerere University, P.O Box 7072, Kampala, Uganda Code Number: js07018 Background: Variations in the number of ribs and vertebrae have been noted in other wise normal looking people with some having supernumerary while others subnumerary. Sternal variations and anomalies though have not been as widely documented. These are two cases with one having a combination of sternal anomalies, supernumerary thoracic vertebrae and ribs and subnumerary lumbar vertebrae while the other had subnumerary thoracic vertebrae and ribs. Introduction Life with fewer numbers of rib numbers started in biblical times when God used one of Adams ribs to create Eve leaving him with eleven ribs1 . Normally, the twelve Ribs and corresponding thoracic vertebrae comprise the thoracic cage which is vital for protection of underlying viscera including the heart, great vessels, lungs, liver, stomach and the spleen. However, it’s particularly important for attachment of the muscles of respiration a vital component of life. Variations in the numbers of ribs and vertebrae have been noted in some cases of other wise normal looking people2-4 . Where there are more denotes a supernumerary and fewer a subnumerary2,3 . This article describes two cases where one has subnumerary thoracic vertebrae and ribs, and another one with supernumerary thoracic vertebrae and ribs but four lumbar vertebrae instead of five, a sternal perforation and an elongated manubrium up to the level of 3rd costal cartilage. Such congenital anomalies occurring in the same individual is so unusual5 . Supernumerary may be associated with teratogenicity of some drugs or chemicals as has been found using experimental animals, but it has been reported in patients with a 22q11.2 deletion6 . These variations are clinically important, especially during diagnostic and therapeutic procedures. Methods These congenital anomalies were discovered during routine preparation of the human skeletons following maceration of the soft tissues at the Galloway Osteological museum of the Anatomy Department, Faculty of Medicine, Makerere University. They were later assembled and reexamined to appreciate and document the variations. Case 1 A 38year old female was found to have eleven thoracic vertebrae and corresponding pairs of ribs after maceration during routine preparation of the human skeleton. The rib cage had upper nine pairs of ribs attached while the distal two pairs were floating. The ribs had normal shape, size, length, orientation and coastal grooves for the corresponding vertebral levels. The eleven thoracic vertebrae were identified by the characteristic features of thoracic vertebrae including heart shaped bodies, small and circular vertebral foramen, long spines that face inferiorly, coastal facets for ribs and large inferior vertebral notches. The vertebrae bodies increased in size from up downwards and the sternum was normal (Figures 1 and 2). Cervical, lumbar and sacral vertebrae were all present and appeared normal in shape, size and numbers, and the rest of the bony components of this skeleton were normal in appearance and other aspects. Case 2 An adult male had thirteen pairs of ribs and corresponding thoracic vertebrae. The vertebrae had the normal characteristics of thoracic nature. The rib cage had eleven pairs that were attached while the 12th and 13th pairs were floating (Figure 3). The manubrium of the sternum was much longer and ended at the sternal angle which was at the same level as the third coastal cartilage attachment and had three costal cartilages attached on either side instead of the usual two pairs. There was an oval deficit in the body of the sternum at the level of attachment for the 5th costal cartilage.Figure 4 The 12th vertebra had no facets for transverse processes but a bifid transverse process and the spine was horizontal and this may be normal because this is a transition area from thoracic to lumbar8. All ribs and vertebrae appeared normal but the lower pair of ribs was completely bone with no costal cartilage at its terminal end, it was much shorter than the other floating ribs and had no costal groove just like the rib above it7. There were four lumbar vertebrae instead of the usual five, and all were of normal shape and appearance. The cervical and sacral segments of the vertebral column appeared normal with no obvious variations or structural deformities and other parts of the skeleton appeared normal. DiscussionVertebral and costal variations are clinically important, especially in diagnostic, therapeutic and spinal anaesthesia involving lumbar puncture where the site of puncture is based on lumbar vertebrae numbers, in cases where there are more lumbar vertebrae, there is likely to be no harm, but in cases where there are few, one can end up injuring the spinal cord8. Since its normal level will presumably be at a lower vertebral level than usual, as the counting is done from L5 upwards basing on the level of the iliac crest. Such can have devastating implications to the patient health wise and the clinician legally. Also fewer ribs can mislead an unsuspecting clinician while doing procedures that depend on counting the number of ribs. Such procedures include; placement of a needle in the 2nd intercostal space anteriorly during emergency relief of a tension pneumothorax and if one has a cervical rib, the doctor can be misled to put it higher in the neck. Placement of a chest tube to draw a haemothorax or an empyema would also be misguided into the pleural space or even causing injury to thoracic viscera or abdominal viscera especially in the developing world where other investigative facilities like X-ray and CT, to mention a few are lacking6,8. Radiological diagnosis that depends on vertebral numbers or rib numbers can be made wrong if the radiologist and or clinician is not conscious of the numbers. Likewise forensic and medical legal pathological identifications need to put into consideration such variations especially where the other party may have had such radiological X-rays of the case in question for proper identification. Knowledge about variation in numbers of ribs and vertebrae is also very essential to students of medicine, radiology, anatomy and forensic pathology. Bone grafting using the twelfth rib will be significantly affected if there are more than twelve or less than twelve ribs; just like location of the kidney using the angle of T12 and L1, approaching the kidney during percutaneous renal biopsy and nephrectomy can be a nightmare8. Extra ribs commonly develop in the cervical and lumbar areas. Fewer ribs may be a result of agenesis of one of the pairs or the 12th during embryological development9. This is associated with trisomy 21, a pair of ribs in the lumbar region is more common than cervical ribs and when present they are usually small. The 12th rib may be absent on one side and shortened on the other, while lumbar ribs also are of great clinical importance in that they confuse identification of vertebral levels in X-rays and other images, that greatly affect positioning of certain clinical procedures. Hence can be mistaken for a fractured transverse process of L1 vertebra. Ribs and thoracic vertebrae comprise the thoracic cage which is vital for protection of underlying viscera and particularly important for attachment of the muscles of respiration which is a vital component of life and the axial skeleton as a whole is important for posture and movement. In the supernumerary case, counting ribs would be very misleading since the manubrio-sternal joint was at the level of third costal cartilage attachment, one below the normal level. This effect will also be a challenge to all procedures that depend on counting of ribs from the sternal angle including; getting reference for the actual site of the apex beat and other valuable levels and for the pleura while doing surgical procedures like pneumothorax and empyema drainage from the chest8. Renal surgery could also be a big problem if the renal angle approach is used in this type of individual because the renal angle is covered by an extra rib. Availability of such knowledge helps the surgeon to devise an alternative approach to nephrectomy and renal biopsy procedures. Interpretation of radiological examination might be confusing because it depends on numbers and site of the vertebrae and ribs present. However, extra protection for the spleen, kidneys and other viscera might be an added advantage to this type of individual hence reducing the effects of direct blows onto these organs. The defect in the body of sternum leaves only the skin separating the pleura and heart from the surface at the affected site, thus any penetrating injury would easily access the heart and cause more severe damage than would normally be. The longer manubrium is unusual and can be both a clinical, radiological and medico-legal challenge when encountered. Supernumerary ribs especially cervical ribs are responsible for thoracic inlet syndrome due to compression of Subclavian artery and lower roots of the brachial plexus C8, T1 which may be a cause of ischemic pain in the arm, forearm or hands and neurological problems. It should be noted that no cervical ribs were discovered in these two cases, but whatever the cause, patients with extra ribs may prove a surgical challenge at the operating table because of the possibility of ending up in different or wrong sites of the mediastinum. The subnumerary lumbar vertebrae encountered in this case is risky in procedures involving a lumbar puncture for diagnostic purposes, spinal anesthesia and therapeutic procedures since possibility of spinal cord being much closer to the level of iliac crest that would lead to its injury especially in children whose spinal cord is at a much lower level than adults. Also the protective cover for underlying organs like spleen and kidneys is reduced hence risk is injury by direct blows over their respective sites. ConclusionsVariations in numbers of both vertebrae and ribs do occur which can be subnumerary or supernumerary, and are important in radiological diagnosis, therapeutic procedures, forensic and medical legal pathological identifications. Knowledge of such variation is essential to students of medicine, radiology, anatomy and forensic pathology just as each variation could have unique features different from others, and could be associated with a number of other congenital anomalies. The discovery of the sternum being different from the usual is important additions to the variations that are expected on the thoracic cage hence need to put this finding in serious consideration during our medical training and practice. Acknowledgements All academic staff department of Anatomy, particulary Drs. Joseph Turyabahika and William Buwembo, Prof. Gabriel R Nzarubara and Godfrey Masilili. Special thanks go to Duncan Kange senior technician for preparing and assembling the specimens. We are grateful to Gertrude Nansimbe for the secretarial services. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07018f5.jpg] [js07018f4.jpg] [js07018f2.jpg] [js07018f3.jpg] [js07018f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}