 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
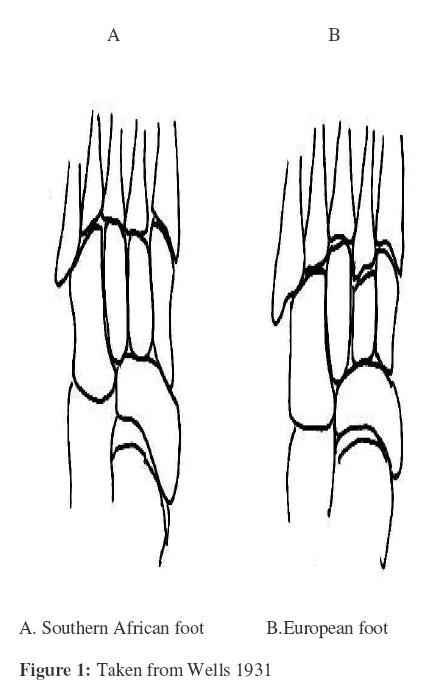
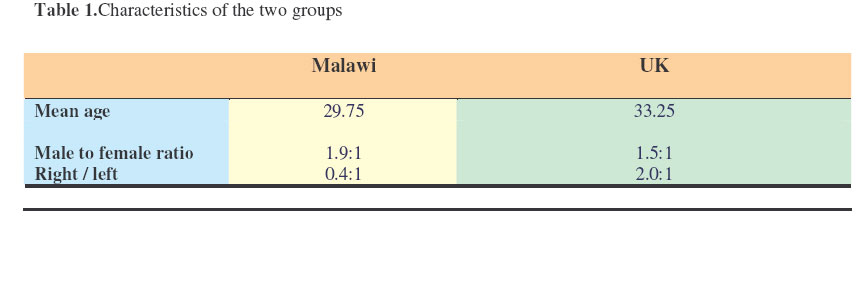
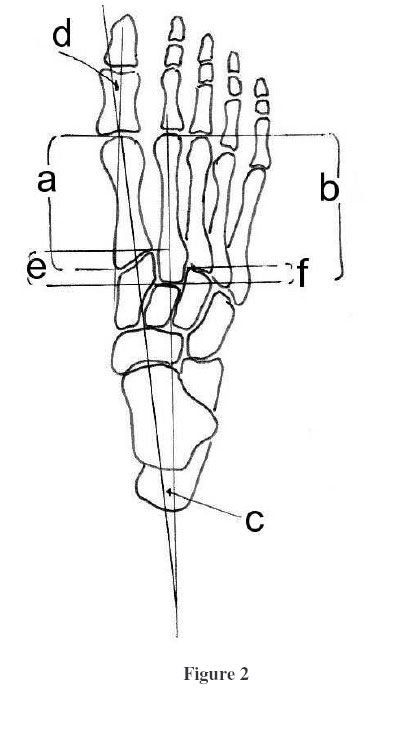
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 105-108 Geographical Differences in the Forefoot Morphology – A Comparative Radiological Study of Feet in Malawi and UK Tindall1, A.; Chokotho2, L.; James3, C. & Lavy4 , C.B.D. 1Orthopaedic SpR, SE Thames Rotation, 2Orthopaedic Clinical Officer, Queen Elizabeth Hospital, Blantyre, 3Orthopaedic Clinical Fellow, Guys Hospital, London,4Orthopaedic Consultant, BTCI Hospital, Blantyre, BTCI Hospital, PO Box 31236, Blantyre 3, Malawi, Code Number: js07019 Background: Many skeletal morphological differences between populations have been reported with possible but unproven clinical importance. This study was aimed at identifying the normal radiographic findings and measurements seen in patients from Southern Africa and compares them to a European population’s values. Introduction Many skeletal morphological differences between populations have been reportedwith possible but unproven clinical importance1,2,3 . In 1931 Wells, in South Africa described the Bantu foot as having less stability than the European foot because of a shallower mortice at the base of the second metatarsal (Figure 1). We were unable to find any other geographical comparative studies of this joint. In 2002, Peicha discussed the anatomy of the second metatarsal and showed that the mortice surrounding the base was shallower in a group of 33 patients who had suffered Lisfranc (tarso-metatarsal) dislocations than it was in a group of 88 cadaveric ‘normal’ feet4 . We decided to investigate Wells’ findings by comparing foot radiographs in Malawian and UK populations. Materials and Methods We retrospectively examined plain anteroposterior radiographs of weight bearing uninjured feet from 40 adults taken at random from hospital radiology department files from the preceding 12 months in London UK and Blantyre Malawi. The characteristics of the patients are shown in Table 1. Each radiograph was placed on a light box and the following measurements carefully performed (Figure 2):
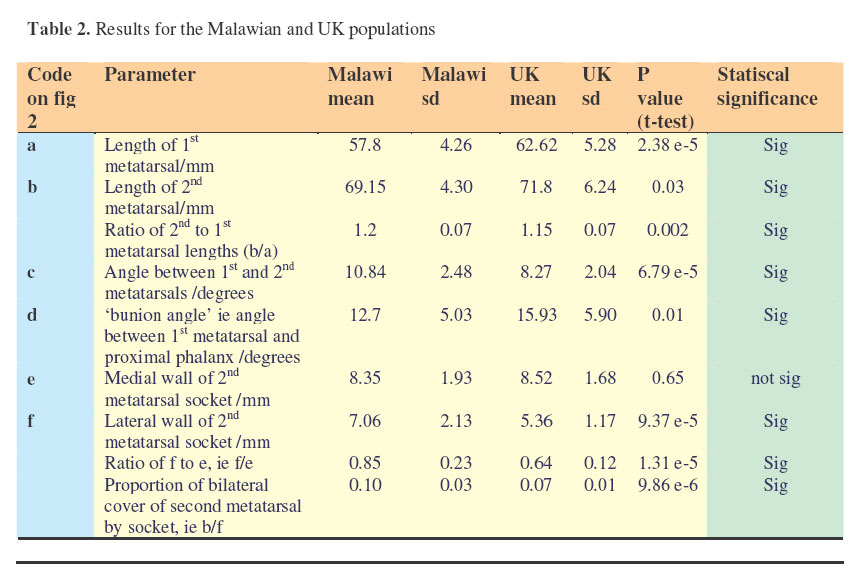
These results were then analysed using Microsoft Excel spreadsheet software. P values of less than 0.05 were considered to be statistically significant. The mean differences between the two groups were tested using Student’s two sample ttest assuming that there is equal or unequal variance depending upon Levenes test for equality of variance after inspection of the data for symmetry of distribution. Results Table 1 summarizes the characteristics of thr two groups. The results of the findings are shown in table 2, which also shows the ratios between the lengths of 1st and 2nd metatarsal bones, both sides of the 2nd metatarsal mortice, and the proportion of the 2nd metatarsal that is bilaterally covered in the mortice. Discussion Foot sizes The overall lengths of 1st and second metatarsals were longer in the UK radiographs. This may be because the population had larger feet, and this is indeed likely as Malawi has regular famines and a high degree of malnutrition. However the lengths of bones on radiographs cannot be accurately be compared between centres as different limb to film distances can distort measurement. Relative length of 2nd metatarsal The 2nd metatarsal length relative to that of the 1st metatarsal was significantly longer in the Malawian than in the UK radiographs. This has not been reported before and is unlikely to have any clinical significance. Angle between 1st and 2nd metatarsals This is significantly larger in the Malawian radiographs and is probably related to unrestrained splaying of the foot when weight bearing, as many people in Malawi do not wear shoes. ‘Bunion’ angle This is significantly larger in the UK population. This is perhaps surprising in view of the bigger 1st/2nd metatarsal angle in the Malawian population; a varus 1st metatarsal is often associated with hallux valgus. It is possible that the lack of shoes allows the metatarsals to splay on weight bearing, and the lack of a varus deforming force on the hallux in the unshod foot reduces the tendency to hallux valgus. Certainly the authors have noticed very few patients in Malawi present clinically with bunions. Cover of the 2nd metatarsal base The proportion of the 2nd metatarsal that is enclosed in the mortice both medially and laterally is higher in the Malawian radiographs (10%) compared to those from the UK (7%). This is the exact opposite to the pattern reported by Wells and on purely anatomical grounds makes the Malawian foot likely to be more stable and less susceptible to a Lisfranc dislocation than a UK foot.5 Conclusion Our study has suggested that the population X-rayed in Malawi have slightly smaller feet than the UK population measured. The Malawi group has a significantly longer second metatarsal relative to the 1st, with significantly more mortice cover at the base of the 2nd metatarsal. Malawian feet also have a significantly bigger 1st / 2nd metatarsal angle and a smaller bunion angle. These differences are probably due to a combination of inherited characteristics and environmental factors such as wearing shoes It is possible that these findings explain the apparent lack of symptomatic hallux valgus. It is also possible that the Malawian foot is inherently more stable to Lisfranc dislocation. AcknowledgementThe authors would like to thank Professor Leslie Klenerman, who suggested the project. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07019t2.jpg] [js07019f2.jpg] [js07019t1.jpg] [js07019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}