 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
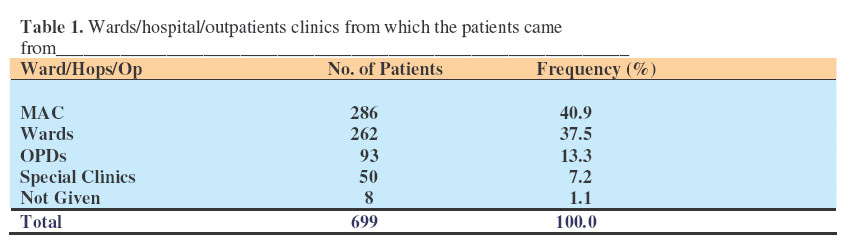
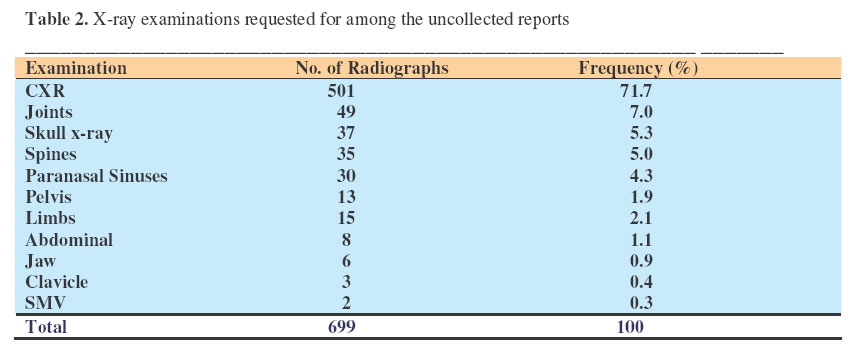
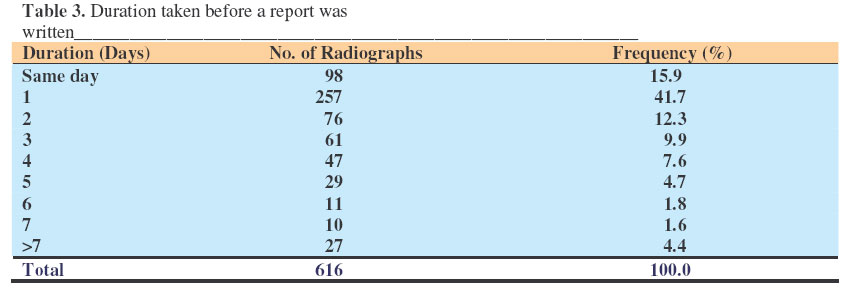
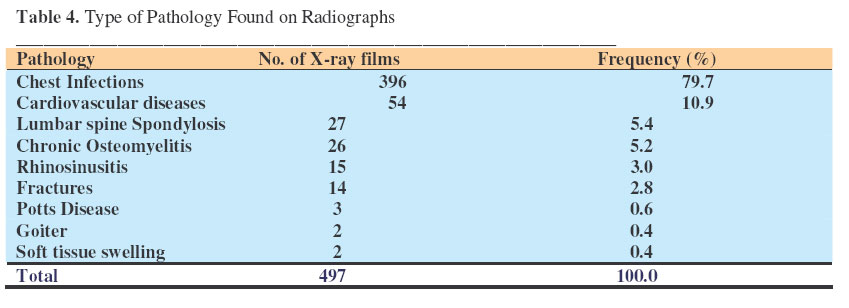
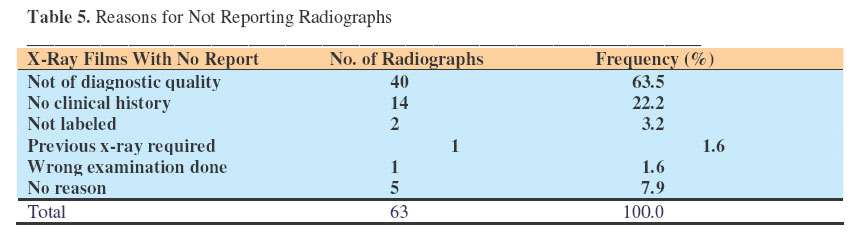
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 109-113 Uncollected Radiographs in a National Hospital with Low Resources. Nabaweesi – Batuka, J. & Kiguli -Malwadde E, E. Department of Radiology, Mulago Hospital, Kampala, Uganda. Code Number: js07020 Background: Communication between clinicians and radiologists is commonly through reports written by radiologists. It is important this information gets to the clinicians if it is to be utilized. Many radiographs remain uncollected in Mulago Hospital X-ray Department. The aim of this study was to establish if uncollected radiographs in Assessment Center x-ray unit had pathology and reports. Introduction The Assessment Center x-ray unit is one of the large x-ray units in Mulago Hospital which is located in the capital city of Uganda. Mulago Hospital is the main teaching Hospital and main National referral hospital. The imaging facilities available include Computerized Tomography (CT), Mammography, Fluoroscopy, generalpurpose x-ray machines and Ultrasound. Facilities available at the Assessment center x-ray unit include: general-purpose x-ray and 2 ultrasound machines. The unit provides free imaging services to the outpatient departments and the wards in upper Mulago Hospital. Currently an average of 75 patients is seen per day. Work normally begins at 8:00am and should be completed by 2:00pm, but may continue till 4pm because of the increasing patient load. The unit has both a radiologist and radiographer as the in-charges. Other staff members include 2 radiologists, 2 senior house officers, 2 nurses, 5 radiographers, 1 sonographer and the support staff. Between March 2001 and July 2004, 70% of 100- 120patients seen each day were x-rayed. During one of the departmental meetings it was noted that many radiographs remain uncollected. Some persons suggested that these radiographs were normal and not collected for this reason. Others suggested the radiographs hadn’t been read and reported upon. Since these reasons were both presumptions it was decided that an audit be performed to determine the facts. Methods This study was carried out in Mulago Hospital, Uganda’s main teaching and National referral Hospital. A radiologist looked at a total of 699 envelopes found in the Assessment Center X-ray archives. These belonged to patients received at the center between March 2001 and July 2004. A precoded questionnaire to record information in a systematic manner was used to collect data. Data was entered into EPIINFO and analyzed using both EPIINFO and SSPS 10software. Results A total of 699 envelopes were got from the archives. The patients came from 26 wards including outpatient clinics. The majority of patients (40.9%) were referred from Medical Assessment Centre (MAC). The ward / clinic was not indicated on 8(1.1%) request forms. (Table 1) Table 2 shows x-ray examinations requested for among the uncollected radiographs. The commonest examination requested for was the CXR accounting for 71.1%. The majority of radiographs 628(90.9%) had been read and reports were present. A total of 63 (9.1%) films had no reports. Eight (1.1 %) envelopes were empty, the patients had been registered, but not xrayed. Twelve (1.7%) envelopes had request forms and reports but no radiographs. Two-thirds of the reports were generated the same day and the next as had been agreed in the department. The median delay was 4days. Twenty-seven (4.4%) films were reported after 7days (Table 3). The majority of radiographs had pathology, the frequency of which is shown in Table 4. The commonest pathology seen was chest infections accounting for 81.2%. Other findings included raised intracranial pressure (1), compensatory emphysema (1), spina bifida (1) Adenoid Hypertrophy (1) and Hirshprung`s disease (1). (Table 4) Radiograph of non-diagnostic quality was the commonest reason why no reports were written accounting for 63.5% of the radiographs with no report (Table 5). DiscussionIn this modern era, most departments have stopped using films and are using Picture Archiving and Communicating Systems (PACS). However, in low resourced countries like Uganda, films are still being used. Unfortunately, many x-ray films remain uncollected in the Assessment centre x-ray unit and yet there is always a limited number of films available. Due to the lack of staff in the Records department, x-ray films are not delivered to the respective clinics or wards but are carried back by the patients. The greatest percentage of patients seen in the Assessment X-ray centre is from the wards in upper Mulago and Medical Assessment Center accounting for 78.4%. The rest of the patients were mainly referred from the outpatient clinics in lower Mulago, which should be the case. In 8 cases the ward/clinic from which the patients were referred was not indicated. The clinical history was inadequately given and only a signature without a name of the referring doctor. This makes it difficult for the radiologist to trace the patients or the referring doctor. The chest x-ray was the commonest examination requested for accounting for 79.7% similar to findings elsewhere in the world1. The majority of radiographs (57.6%) were reported within 24hours, as is the policy of the Radiology Department at Mulago Hospital but still a significant number of radiographs were reported after 24hours. The main reason for the delays is the few radiologists on the ground and yet the workload has markedly increased. In order to provide an appropriate and quick service to the patients and referring clinicians, the radiology capacity needs to match the demand2,3 . It is also important to establish that the requests made by the clinicians are appropriate and provide all the information required for a good report to be written4,5 . Radiographs are sometimes given out to patients without reports to reduce on the delays but the doctors later send them back for a report6. This explains why some reports were written after 1week. As a way of reducing on the delays and over coming the shortage of radiologists, radiographers could have extended roles like report writing7,8,9,10. Some have already been trained in ultrasound and are writing reports. They could also be trained in film interpretation so that the burden on the few radiologists is reduced. Safeguards should however be in place and these include agreed protocols and proper training11,12,13 . Most radiographs had reports and the majority had pathology contrary to what had been presumed; that the uncollected radiographs were normal and had no reports. The various reasons as to why no reports were written included:
In 5 (7.9%) cases no reason was given. The above shows a lot of film wastage and yet there is always a limited amount of consumables provided especially the x-ray films. The reason for non-diagnostic radiographs could be due to the breakdown of equipment at certain times; x-ray examinations are then taken using small portable x-ray machines. Eight patients were received and registered but were not x-rayed. These were probably patients who were not patient enough to wait or were taken elsewhere for a “quick” service. In some cases the x-ray films were used up and yet the patients had already been registered. The misplaced radiographs in the 12 cases reflect a weakness in the archiving system. ConclusionThe majority of uncollected radiographs in the Assessment Center X-ray unit at Mulago Hospital had pathology and reports. The fact that they were not collected deprived patients and clinicians of important information that may have had impact on the care and disease progress. Further research into the causes of non-diagnostic radiographs needs to be carried out. The hospital management and medical staff must institute means to monitor and change this problematic situation via quality assurance programs. Recommendations
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07020t3.jpg] [js07020t4.jpg] [js07020t2.jpg] [js07020t5.jpg] [js07020t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}