 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 114-119 Experience of Pericardiectomy in Tikur Anbessa University Hospital, Ethiopia Ali, Adem; Biluts, H. & Bekele, A. Thoracic surgical unit, Tikur Anbessa Hospital, Department of Surgery, Medical Faculty, Addis Ababa University, Addis Ababa, Ethiopia Code Number: js07021 Background: Pericardiectomy is the only accepted curative treatment for improving cardiac haemodynamics in chronic constrictive pericarditis (CCP). This study was aimed at reviewing the experience and functional outcome of patients undergoing Pericardiectomy in Tikur Anbessa Hospital between January 1996 and December 2005. Constrictive pericarditis (CP) is an uncommon disorder with various causes1,2 . Chronic constrictive pericarditis (CCP) is a chronic inflammatory process of pericardium, leading to pericardial fibrosis and thickening that restricts diastolic filling of the ventricles3-5 . Tuberculosis(TB) was a leading cause in the past, but most are cases now idiopathic or follow prior radiation therapy or operation6,7 .Yet TBC remains a leading cause of pericarditis in some nonindustrialized countries8,9 ,such as those of sub- Saharan Africa8-10 , where infection with human immunodeficiency virus (HIV) has become pandemic. In Ethiopia only one report on Pericardiectomy for constrictive pericarditis was found by Johonson11. Tuberculous pericarditis affects 1% to 2% of all patients with TB by direct extension from the mediastinal lymph nodes and, occasionally, by haematogenous spread or by contiguous spread from the myocardium8 , 12 .Tuberculous is responsible for approximately 4% of cases of acute pericarditis, 7% of cases of cardiac tamponade, and 6% of instances of constrictive pericarditis13 . Accurate diagnosis is essential as pericardiectomy is the only effective treatement4,5,14 . A variety of surgical approaches have been described, including left anterior thoracotomy, bilateral thoracotomies, or median sternotomy. Best exposure is usually provided by the latter3,12,15 In Ethiopia only one report on Pericardiectomy for constrictive pericarditis was found by The purpose of this study is to review our experience of pericardiectomy in patients with constrictive pericarditis in Tikur Anbessa Hospital between January 1997 and December 2006. Patients and Methods:Of 26 patients who had undergone pericardiectomy in Tikur Anbessa Hospital between January 1996 and December 2005, the medical records of 19(73.1%) patients were retrieved and included in the study. Data concerning socio-demographic status, clinical manifestations, diagnostic studies, operative procedures, post operative course final out come and histological examination results of pericardium were recorded in the structured format. Analysis was done using computer based statistical software SPSS version 11.0. Diagnosis of CP was based on the clinical picture of right sided heart failure complimented by chest roentgenogram, echocardiography, Doppler echocardiography and electrocardiogram findings. All patients had received chemotherapy for tuberculosis before the present admission. Pre and postoperative New York Heart Association (NYHA) functional classification was done to assess early postoperative out come of pericardiectomy. The extent of decortication of the pericardium varies from a procedure that decorticates:
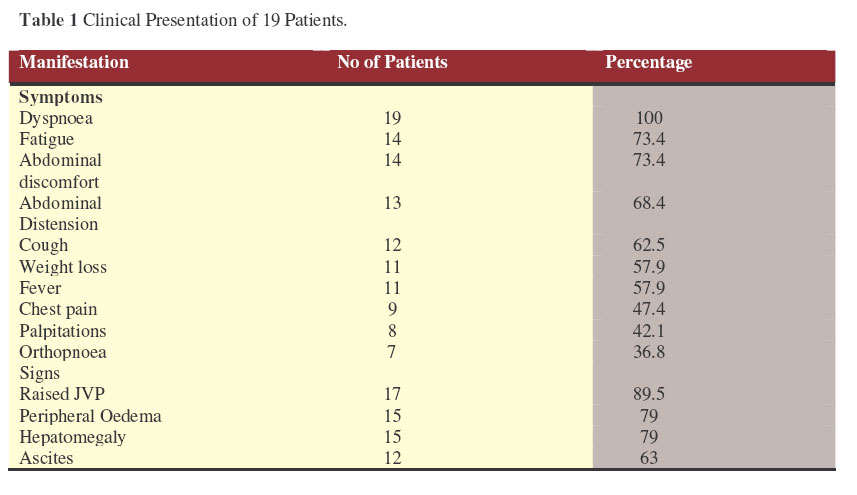
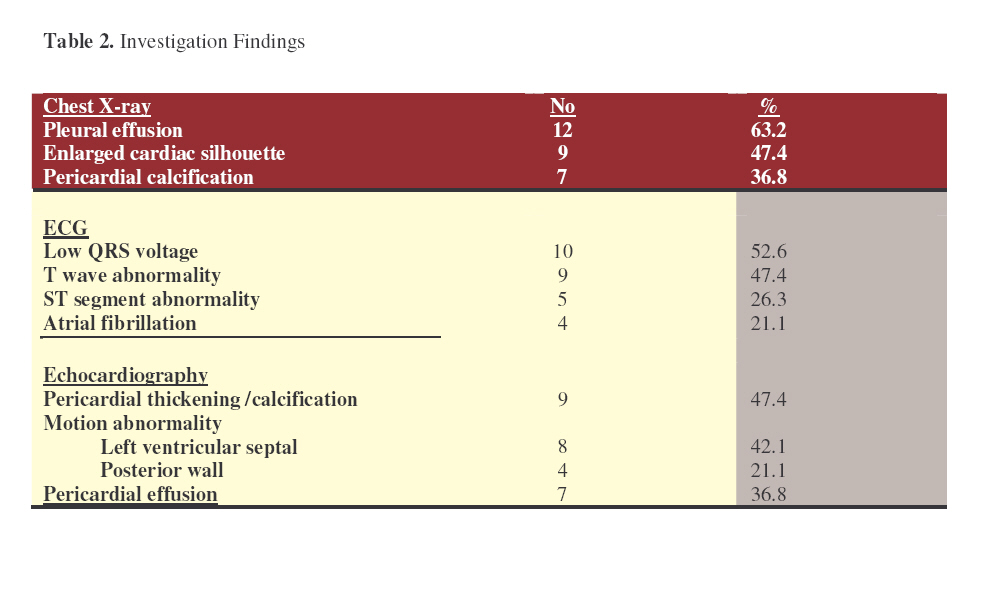
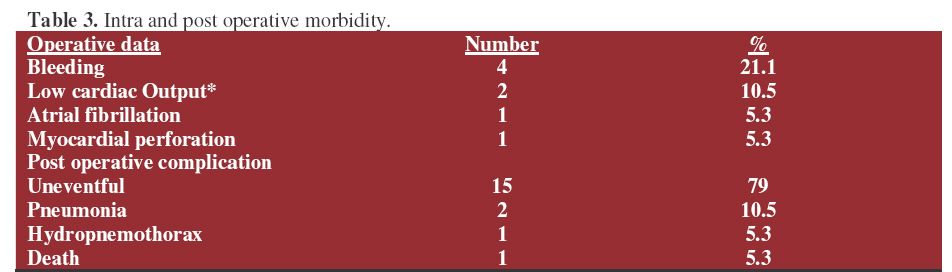
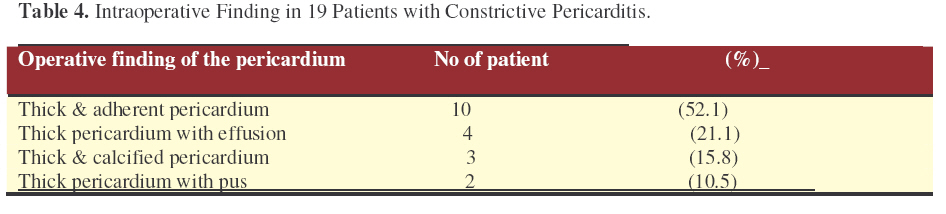
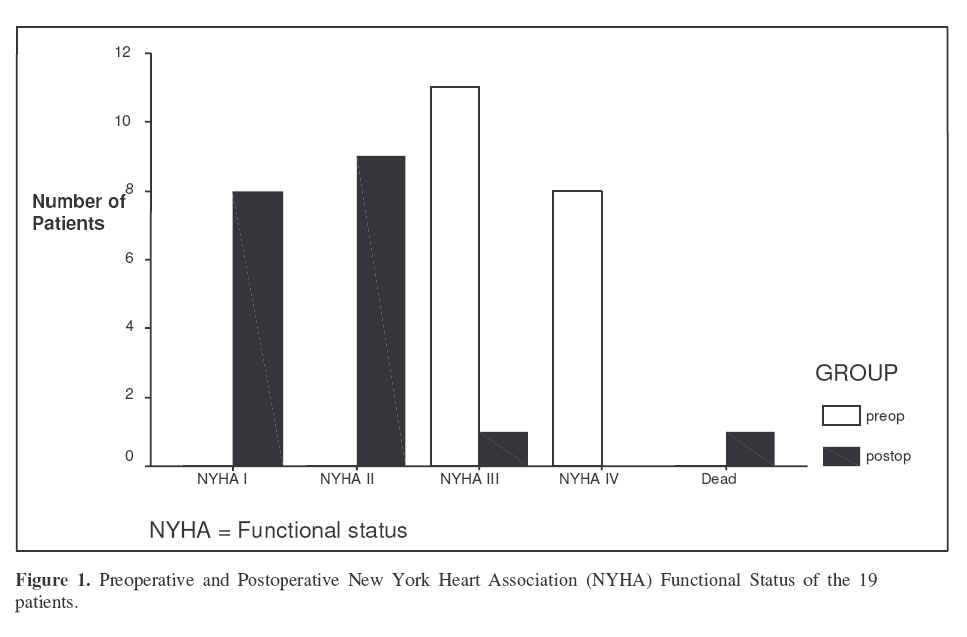
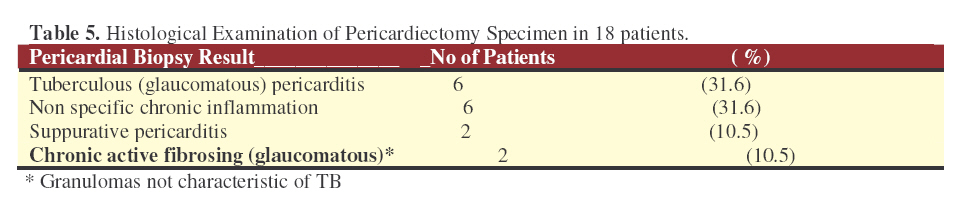
Resected pericardium was subjected for histopathological examinations. ResultsThere were 13 males, 6 females (M: F ratio = 2.2:1), mean age 24.3±7 years (range 14-42). Duration of illness prior to admission to surgical ward for pericardiectomy ranged between 2-36 months (mean 15.2±10.8). Dyspnea (100%), fatigue (75%), abdominal discomfort (73.7%) and abdominal distension (68.4%), raised JVP (89.5%), hepatomegaly (79) and ascites (63%) were the most common clinical presentation of patients with constrictive pericarditis (Table 1). Physical examination of the heart in the majority of cases revealed distant / soft heart sound, soft & diffuse apical impulse (quiet precordium) and pericardial knock was heard in one-quarter of the patients. On electrocardiography, low QRS voltage was detected in half of the patients, T wave abnormality and atrial fibrillation was found in 9 and 4 patients respectively (Table 2). Echocardiography showed pericardial thickening / calcification in 10 (52.6%) patients, left ventricular septal motion abnormality in 8 (42.1%) and pericardial effusion of different degrees in 7 (36.8%). The mean ejection fraction was 0.55.7±11.7 (range 0.27-0.65), as determined by echocardiography. Chest radiography showed pericardial calcification in 7 patients (36.8%), enlarged cardiac silhouette/cardiomegaly in 9 (47.4%) and pleural effusion in 12 (63%). In 15 patients (79%), pericardiectomy was performed through median sternotomy and in 4 (21%) through left anterolateral thoracotomy. Extent of pericardiectomy was subtotal in all patients. Thick pericardium was the classical finding in all cases of pericardiectomy. Pericardial effusion and calcification were seen in 21.1% and 15.8% of the cases respectively (Table 4). Non-fatal intraoperative complications affected 8 patients (42.1%). However there was one patient who continued to have low-output syndrome beyond the intraoperative period and died secondary to severe low-cardiac-output syndrome despite resuscitation with catecholamine, dopamine, and blood transfusion. Postoperative complications; and condition of patients during discharge and follow-up are shown table 4 and 5 respectively. One of the eighteen surviving patients was readmitted 4 years after pericardiectomy and died from complications of post TB fibrothorax and persistent pericardial constriction. Marked improvement in 13 (87%) of the 15cases and long-term mortality in 2 (13%) during follow-up period were noted. Postoperative outcome was compared using the New York Heart Association (NYHA) functional status. Preoperatively, there was no patient in class I or II, 11(58%) in class III, 8 (42%) in class IV (Figure 1).Postoperatively 8/18(45 %) patients were in class I, 9/18(50%) in class II. The mean stay in the intensive care unit pulmonary TB and other focus of tuberculosis. Microscopic examination of the excised pericardium showed and duration of post operative hospitalization was 3.38 ±1 (range 2-5) and 14.3±5.3 (range 7-24) days respectively. All patients received antituberculous therapy preoperatively and in the postoperative period. Preoperative indications for anti-TB treatment were TB pericarditis, Table 5 shows the histological findings of the pericardiectomy specimens in 18 cases. Tuberculous pericarditis was diagnosed in 6 cases. There were 6 non-specific chronic inflammatory specimens and 2 cases of suppurative pericarditis (Table 5). Five had been treated for proven TB of the lung or pericardium in the medical ward prior to admission to surgical side. Four patients had HIV/AIDS in addition to tuberculosis. Discussion The occurrence of chronic constrictive pericarditis in the young age group (mean 24.3±7 years) is similar to O.Johonson’s review and others11,12,15 but our patients are significantly younger than the patients reported by Bozbuga N (2003) and Abdelmeguid I (2002) (p<0.001), who reported mean age of 32.2 and 35 years respectively. In agreement with many reports, our results showed predominance of males over females. The interval from surgery to presentation varies in different series, 1< to >4 years by Johonson, mean of 23 months by Killian and 2.3(range 0.5-6) years by Bozbuga11,12,16 . Duration of complaints in our review was 14.5±12.8months. Pericardiectomy is the only accepted curative treatment for improving cardiac hemodynamics in CCP. It may be difficult to distinguish constrictive pericarditis from restrictive cardiomyopathy. Every effort should be directed to confirm the diagnosis, eliminate other causes of right sided failure and determine its etiology 12,1719. The clinical presentations of our patients were in agreement with previous reports11,12,15 . The diagnosis CCP was clear in all patients, symptoms and signs of right heart failure, low QRS voltage in electrocardiography (52.6%), pericardial thickening/calcification in echocardiography (42.1%), cardiomegaly and pericardial calcification seen by chest roentgenogram in 36.8% and 31.6% patients respectively. Moreover, intraoperatively, the finding of thickened pericardium in all cases was in favour CCP. Although tuberculosis was considered as the main cause of CCP, most cases are now idiopathic or follow prior radiation therapy or operation6,7. But still TB is the most common cause of pericarditis in some developing countries (8, 9).In our group of patients, a total of 11(75%) patients were diagnosed to have TB CP, six proven TB pericarditis on histological examination, five treated for clinically proven TB of the lung, pericardium or both. Indications for operation were effusive disease in 7 patients and constriction in 12 patients. Regardless of the surgical approach or use of cardiopulmonary bypass, investigators have reported normalization of cardiac haemodynamics after total or subtotal pericardiectomy15,20,21 . Median sternotomy and left anterolateral thoracotomy were used in 15 and 4 patients respectively. The amount of pericardium to be decorticated is a matter of controversy, but most surgeons advocate a procedure that decorticates all the right and left ventricles from phrenic to phrenic, including the anterolateral and diaphragmatic surfaces. Resection of pericardium overlying the atria or vena cavae probably adds little haemodynamic benefit but reported to increase the risk of bleeding complications3.Total pericardiectomy was considered as wide excision of the pericardium from all surfaces of the heart and major intrapericardial vessels; with the phrenic nerves defining the posterior extent of pericardial resection.Whereas subtotal pericardiectomy was defined as decortication of the constricting pericardium from both ventricles without the removal of pericardium overlying the atria and venae cavae. In this review, all patients had subtotal pericardiectomy. All patients were operated without the use of cardiopulmonary bypass. Most surgeons do not or rarely use cardiopulmonary bypass; standby machine may be primed in patients with concomitant heart operations, and low ejection fraction12,15 . Both Bozbuga et al12 , Abdelmeguid et al15 reported a 30-day operative mortality rate of 6%, while McCaughan18 reported 5% to 15%. Theses findings are in accordance with our in-hospital and long-term mortalities of 5.6% and 10.5% respectively. The mean stay in-hospital and intensive care unit were also similar to that of Bozbuga and others12 . At the 1-year follow-up, improved functional status was noted in 94% of the surviving patients which is similar to other reports12,15 . In conclusion, Pericardiectomy is a gratifying procedure that can be performed in an environment where cardiopulmonary bypass is unavailable, resulting in low mortality and improved functional capacity of the heart in the majority of the patients. Acknowledgments:We would like to thank the department of surgery for the support to undertake this study. Special thanks go to Dr Dereje Gulilat (M.D), who was in charge of some of these cases References:
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07021t1.jpg] [js07021t4.jpg] [js07021t5.jpg] [js07021f1.jpg] [js07021t3.jpg] [js07021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}