 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
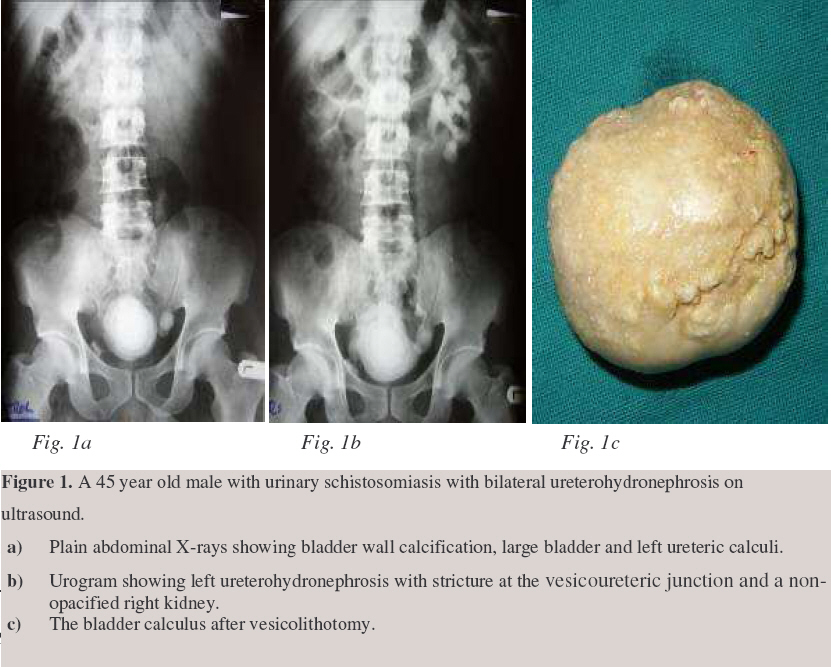
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 120-125 Surgical Aspects of Genitourinary Bilharzia Maranya, G. A.; Al-Ammary, Y.A. & Oduor, P. R. Consultant Surgeons, Coast Province General Hospital, P.O. Box 91066-80103, Mombasa, Kenya Code Number: js07022 The blood fluke Schistosoma haematobium mainly affects the lower genitourinary tract, where the pathological effects are a result of the reaction to the schistosome ova. The chronic effects cause damage to the musculature of the urinary tract resulting in scarring and fibrosis. The ureters dilate and or stricture. Contracture of the bladder and or detrussor failure may occur. Secondary calculi in the upper tracts and bladder are common. There is strong association with bladder cancer development of the squamous cell type. Emphasis is on the prevention of the infestation. IntroductionInfestation with the blood fluke Schistosoma haematobium is endemic in Eastern, Central and West Africa, Egypt and the Indian Ocean islands off the Eastern Coast of Africa. It is transmitted through contact with contaminated water1. The causal agent of genitourinary schistosomiasis was described in 1851 by Theodor Bilharz when he found a blood fluke in a mesenteric vein during a postmortem examination in Cairo, Egypt1. The schistosomulae (larvae) of the Schistosoma haematobium develop in the portal vein of the infected human host. At maturity the coupled adult worms migrate to the veins of the vesical and pelvic plexuses where they mate and the female lays eggs. Involvement of the various urogenital organs varies and appears to correlate with the extent of their venous circulation. The urinary bladder, lower ends of the ureters and seminal vesicles are most commonly affected by the disease in view of their rich venous supply2. PathologyThe pathological effects of Schistosoma haematobium infestation in man are mainly the result of an intense host reaction to the eggs. The main target organs are the bladder, distal ureters, the prostate, seminal vesicles and the spermatic cords3. Initially granulomatous lesions form in the lamina propria. The extent of the lesions, their healing, progression, or complication depends on the tissue egg load, the frequency of re-infestation, the efficiency of treatment and the onset of secondary infection. There was a significant correlation between egg burden and the histological severity of tissue reaction2. The Upper Urinary TractsThe endopelvic part of the ureters is principally involved. The eggs may be found in all layers of the ureter. The end result is healing with a variable degree of mural fibrosis with loss of muscle and development of peri-ureteral adhesions. The sum of these changes is an obstructive uropathy caused by stricture formation and or atony and dilatation of the involved segment (Figure 1). Tissue egg loads are greater in cases with obstructive uropathy than in those without4. Vesicoureteric reflux has also been reported. Eventually, urinary stasis invites secondary bacterial infection and stone formation (Figures 1, 2, 3). Anuria5 results from bilateral total ureteric obstruction mainly by stricturing which may be aggravated by secondary calculi (Figure 2). ManagementEndourology may be useful for early short segment strictures. This entails endoscopic dilatation and visual internal urethrotomy6. In anuria this mode of intervention may be tried first. If it fails, nephrostomy is performed followed by further evaluation and appropriate surgery. Open surgery is indicated for more established lesions.
Urinary Bladder Acute schistosomal effectsAtrophic changes result from heavy submucous ova deposition with subsequent reduction of the blood supply to the overlying epithelium. Secondary infection may play an aggrevating role, resulting in erosion of the surface epithelium, thus forming bilharzial ulcers2. Other effects are: haemorrhagic cystitis, acute erosions, granulomatous polyps, and pseudotubercles. Endoscopic examination is critical in evaluating these bladder lesions. Adequate therapy with anti-schistosomal medication results in favourable healing with reversal of granulomatous lesions, small amount of mucosal fibrosis and dystrophic calcification9. Chronic effects.These are mainly the result of fibrosis and reduced vascularity of the bladder wall3. They include sand patch lesions, chronic ulcer, cystitis cystica and glandularis, leucoplakia, bladder neck stenosis, bladder contracture, bladder hypotonia and bladder carcinoma3. Most of these lesions can be ascertained by endoscopic evaluation. A plain X-ray may show bladder wall calcification (Figure 1a), but this per se does not affect bladder function.
Since secondary bacterial infection is common in bladder schistosomiasis, stones can develop as a result of infection by specific organisms that secrete the enzyme urease12.The consequent hydrolysis of urinary urea produces ammonia. The presence of ammonium ions and high pH induce the production of stones containing calcium, magnesium, and ammonium sulphate. Stones produced by urea-splitting organisms are often very large (Figure 1). There is usually no associated bladder outflow obstruction. Treatment is by endoscopic cystolitholapaxy or open vesicolithotomy. Carcinoma of the bilharzial bladder.Bladder carcinogenesis is probably related to bacterial and viral infections, commonly associated with bilharzial infestation, rather than the parasite itself13 . Urinary bacteria have a double action, namely (i) secretion of β-glucuronidase enzyme which may clear conjugated carcinogens, yielding free carcinogenic products, (ii) the production of carcinogenic nitrosamines from their precursors in urine, such as nitrates and secondary amines14 . Local mechanical irritation by Schistosoma eggs appears to be an important promoting factor13 . Two thirds of the cancers show squamous cell differentiation15, 16. This tumour is of high grade, invasive and more aggressive than transitional cell carcinoma. Most patients present for treatment at an advanced stage. The explanation for the late presentation may be the overlapping of symptoms of simple bilharzial cystitis with early malignant cystitis13 . The diagnosis depends on cystoscopy, biopsy and careful bimanual examination under anaesthesia13 . Treatment
Occasionally bilharzia affects the bulbous urethra and may result in peri-urethral abscesses, fistulae or stricture formation2. Bilharzial seminal vesiculitis may result in haemospermia, painful ejaculation and low back pain, just as may bilharzial prostatitis. Plain x-ray may show calcification in the seminal vesicles with a honeycomb appearance. Infestation of these organs has no effect on fertility2. Schistosoma haematobium has been found in the cervix, vagina and vulva. There is an increased incidence of infertility in this group1. Prevention and ControlPrevention of Schistosoma haematobium infestation1 can be achieved by:
Bilharzia can be controlled by simple measures, which with determination, can be effected by the community and the Government. It is the hope of the authors that this will be achieved and even result in the eradication of this parasite in our continent of Africa and thus consign this publication to the archives of surgery. AcknowledgementWe are sincerely grateful to Jason Mwawana for the computer work. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07022f3.jpg] [js07022f1.jpg] [js07022f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}