 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 131-138 Rapid Resuscitation with Small Volume Hypertonic Saline Solution for Patients in Traumatic Haemorrhagic Shock. Sakwari1, V. ; Mkony2,C. & Mwafongo3, V.Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania.1Resident in Anaesthesiology, 3Associate Professor of Anaesthesiology; 2Associate Professor of Surgery,
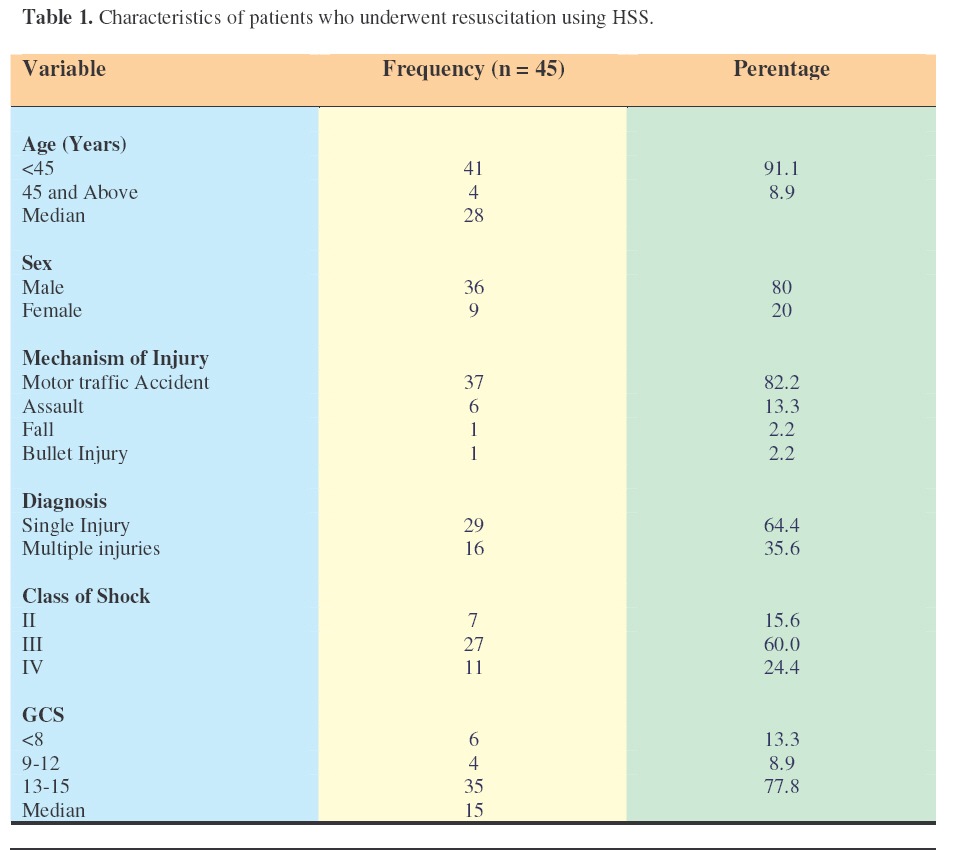
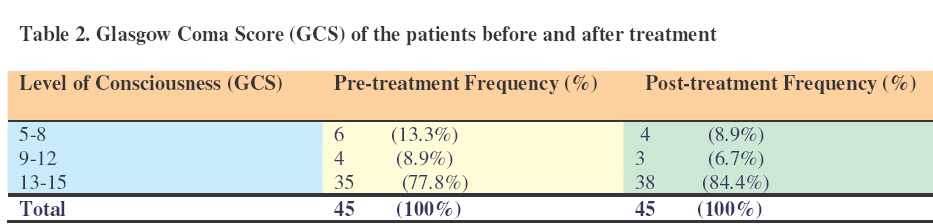
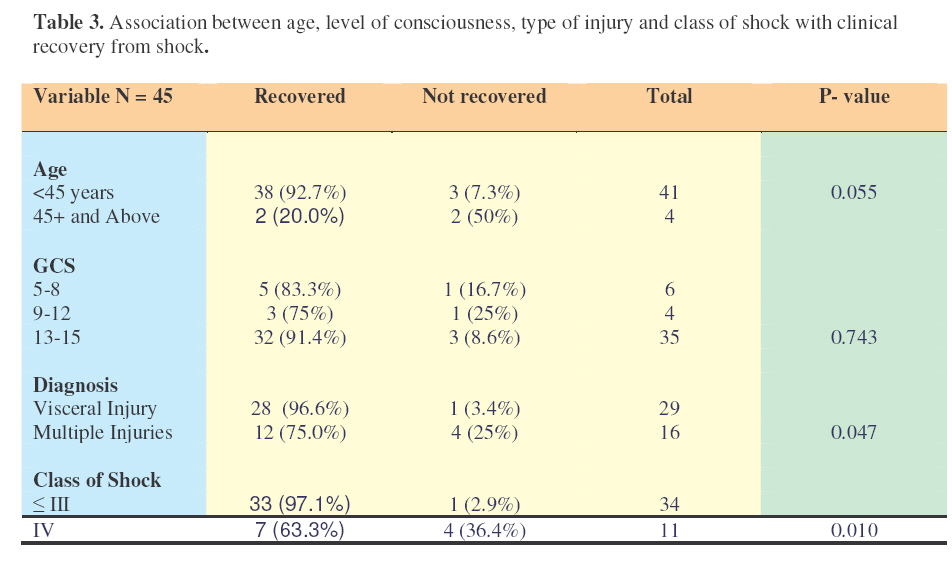
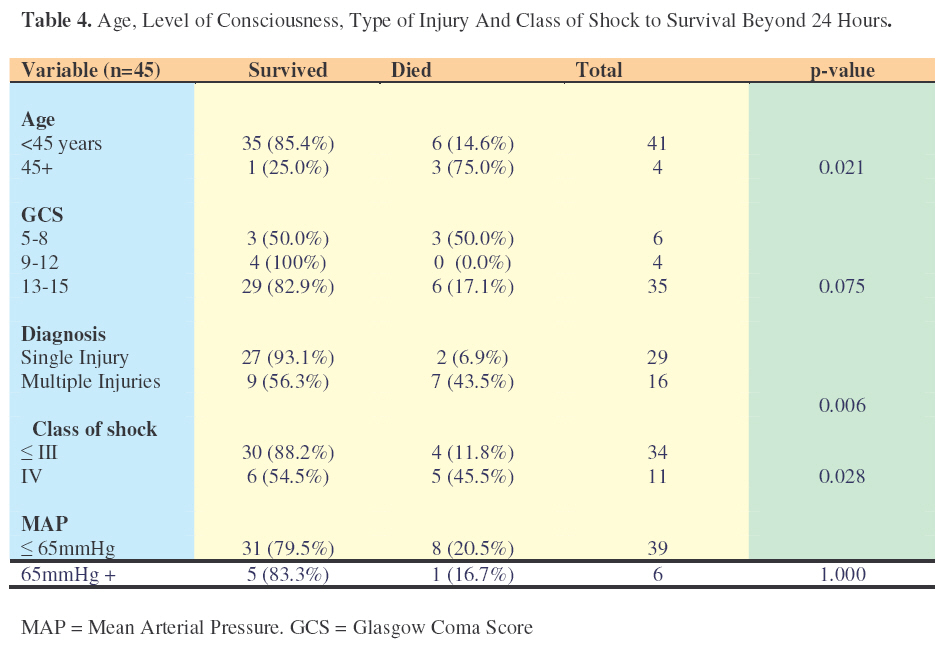
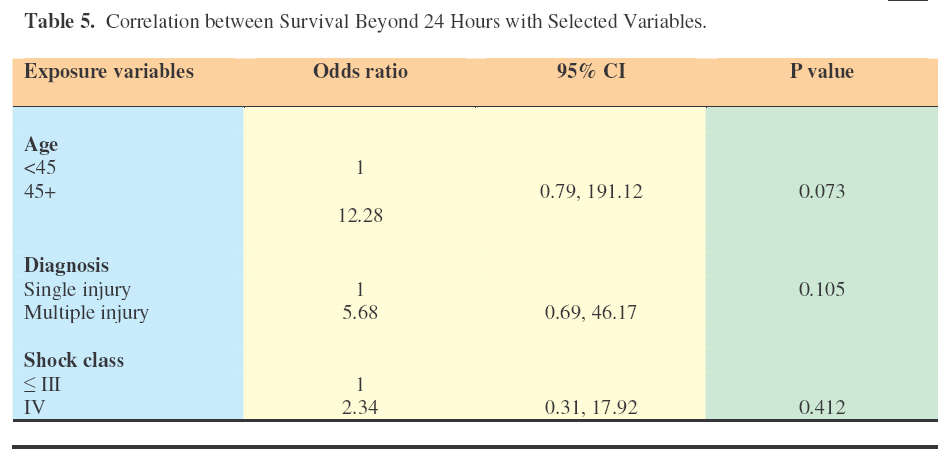
Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania. Code Number: js07024 Background: Haemorrhagic shock is a major cause of morbidity and mortality worldwide. Trauma and its complications account for one in ten deaths worldwide and are the leading cause of death in those below 45 years of age in developed countries. Survival of the shocked patient is influenced by the speed and efficiency with which resuscitation is carried out. Rapid infusion of a small volume of 7.5% hypertonic saline (HSS) has been shown to result in immediate restoration of circulating volume and tissue perfusion but results of investigation of its use remain inconclusive. The objective of this study was to determine the clinical outcomes of infusing locally made 7.5% HSS in patients with haemorrhagic shock. Introduction The earliest use of hypertonic saline solution (HSS) for patient resuscitation was described some 25 years ago. Interestingly, current use of HSS was initiated by a nursing error when a Brazillian nurse inadvertently gave an unconscious shocked dialysis patient 100mls of 7.5% saline, whereupon a minute later the patient regained consciousness and a normal blood pressure1. Subsequently experimental2,3 and clinical research 4,5,6,7,8 work has led to acceptance of the use of HSS for resuscitation in clinical practice 9,10 . Hypovolemic shock resulting from haemorrhage is a major cause of morbidity and mortality worldwide. Trauma and its sequelae account for 10% of global mortality and are the principal causes of death in those below 45 years of age in developed countries11 . A study of trauma deaths in a large North American city revealed that 60.5% of all deaths occurred before victims were hospitalized 12 . It has also been shown that exsanguination is the cause of death in 31 to 39% of trauma deaths, and the proportion is higher if the complications of haemorrhagic shock are included 11,12 . In developing countries gynaecologic and obstetric bleeding is still a common cause of hypovolemic shock 9 . The approach to a hypovolemic patient aims at prompt diagnosis of the presence of shock and its aetiology, rapid restoration of tissue perfusion and prevention of end organ failure 13,14. After securing the airway and excluding any lifethreatening conditions, standard initial treatment requires fluid replacement with crystalloids or colloids. The amount infused depends on the severity of shock and should aim to expand intravascular volume by approximately the estimated blood loss. Different types of fluids expand the intravascular volume differently 14,15 . An infusion of 1000mls of Ringer’s lactate (RL) or normal saline in an adult, for instance, (NS) expands the intravascular volume by approximately 250 millilitres within one hour after injection. Five hundred milliliters of Dextran 70 expands the intravascular volume by 500mls. Five hundred milliliters of 6% Hetastarch expands the intravascular volume by approximately 800 mls in one hour and is sustained for at least 8 hours. Rapid infusion of 250mls of HSS expands the intravascular volume by approximately 750 to 1000mls in 2-5 minutes, sustained for at least 30 minutes. The hypoxia of hypovolemic shock leads to endothelial and erythrocyte oedema, capillary narrowing and impaired blood flow, tissue ischaemia and cell death 16,17 . Mobilization of water from the intracellular compartment has a double advantage: increasing plasma volume and increasing vascular luminal diameter. Infusion of 4mls/kg of HSS within 2 -5 minutes leads to hyperosmolality of the extracellular fluid compartment and mobilization of intracellular water into the extracellular space by osmosis of up to four times the infused volume 1,3,4,6,11 . Numerous studies have demonstrated the desired fluid mobilization into the intravascular compartment (IVC) causing plasma volume expansion18,19,20,21 . Other effects due to HSS infusion include improved cardiac contractility, reduced blood viscosity, improved microcirculation and immunomodulation 20, 22 . A study by Younes demonstrated a significantly higher 24 hour and 30 day survival for haemorrhagic shock patients given HSS than those on standard treatment 24,25 . A Cochrane Library review of 16 randomised trials involving 837 patients concluded that the data was insufficient to decide whether HSS was better than isotonic crystalloids for resuscitation of trauma and burn patients, and for patients undergoing surgery 11 . To date there has been no evidence demonstrated of clinical signs of hyperosmolality due to HSS infusion. 5,6,20,23,26,27. Following HSS infusion the raised serum osmolality starts dropping after 4-8 hours, and is back to normal in 24 hours. HSS infusion for resuscitation has become an established treatment of haemorrhagic shock in hospitals in developed countries, and is being proposed for use in emergency rooms and ambulances. In developing countries patients in need of resuscitation for hypovolemic shock are numerous, the cost of standard infusion fluids is high and the fluids are not readily available. Trauma victims and other patients in hypovolemic shock take much longer to reach hospital due to underdeveloped infrastructure. There are therefore compelling reasons to advocate local studies of the use of HSS in resuscitation of patients in hypovolemic shock. ObjectivesThe objective of the study was to document the immediate clinical outcomes in patients with haemorrhagic shock following resuscitation with locally made 7.5% hypertonic saline. Patients and MethodsThis was a hospital based descriptive study conducted at the Muhimbili Orthopaedic Institute (MOI) Casualty Department in Dar es Salaam, Tanzania. The institute is the main centre for handling trauma cases in the city of 3.5 million inhabitants and is also a national trauma referral centre. MOI houses the academic department of Orthopaedics and Traumatology of Muhimbili University College of Health Sciences. Ethical clearance for the study was granted by the college ethical committee. During the six-month period, July 2005 to December 2005, all adult (age 14 to 70) trauma patients diagnosed with haemorrhagic shock were enrolled into the study. Using a statistical formula the sample size was calculated as 20 patients. Informed consent to be enrolled in the study was obtained from the patient or from a responsible relative in case of patients with impaired consciousness. Patients were excluded from the study if they were pregnant, if they were on fluid infusion or blood transfusion before or on arrival, or if consent was not given. A datasheet designed by the authors was used for patient information, which included identifying data, clinical findings, cause and class of shock, noninvasive measurements of haemodynamic state, haematocrit, haemoglobin, serum electrolytes, serum creatinine, and survival 24 hours after resuscitation. A clinical diagnosis of traumatic haemorrhagic shock was made if the patient with a history of traumatic haemorrhage had a systolic BP of 90mmHg or lower, mean arterial pressure (MAP) of 70mmHg or lower, a pulse rate of more than 100 beats per minute, or urine output of less than 0.5 mls/kg/hr. A patient was considered to be recovering from shock if one or more of the following was documented: SBP >90mmHg, MAP >70mmHg, pulse rate <100bpm, peripheral oxygen saturation >93%, and a urine output >0.5mls/kg/hr. A detailed clinical evaluation was performed. The airway was assessed and secured and oropharyngeal suction performed as indicated. The respiratory rate was recorded before and after HSS administration. Circulatory assessment included a record of the pulse rate, heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP). Five mls of blood was drawn from the anterior cubital vein before commencement of resuscitation for determination of haematocrit, haemoglobin, serum sodium, serum chloride, and serum creatinine. Three to five minutes after HSS infusion, another sample of 5mls of blood was drawn from the contralateral vein. In patients with injury involving the arms the blood was drawn form the femoral vein. Blood was not drawn from the arm in which the HSS had been administered. A urethral catheter was inserted for monitoring hourly urine output. The peripheral oxygen saturation was monitored continuously with the CSI Criticare 504 Dx digital pulse oxymeter. The SBP, DBP and MAP were measured with the CSI Criticare 506 N digital sphygmomanometer. The pulse pressure was determined as the difference between SBP and DBP. The first reading of the vital signs was taken before the HSS infusion and the second 3-5 minutes after HSS infusion and before any additional fluid infusion. All casualty doctors were trained by the authors to comply with the study protocol on resuscitation of trauma patients before commencement of the study. For resuscitation 250mls of 7.5% hypertonic saline per bottle, prepared at the hospital pharmacy was infused through a gauge 16 cannula. Six patients had gauge 18 cannula because of difficult access with a gauge 16 cannula. The 250mls of 7.5% HSS was administered over 2 to 4 minutes. Patients who responded favourably to the HSS infusion were maintained on crystalline intravenous fluids. Those patients who after the initial infusion of HSS had SBP <90mmHg, MAP <70mmHg, with other clinical signs including tachycardia (pulse rate >100/min) were considered as not clinically responding to the HSS infusion. An infusion 500mls NS or RL was commenced to run over 4-6 minutes, repeated as required for the patient to respond to treatment of shock. Blood replacement was carried out when indicated. Meanwhile, preparation was made for surgery and other treatment for the patient’s clinical condition as indicated. Patients were reviewed by attending staff four hourly or more frequently as required. All patients were re-evaluated and findings documented at 24 hours after resuscitation. The degree of shock was classified according to Modified Classification of Shock from the Committee of Trauma of the American College of Surgeons. The data were entered into a computer data base and analysed using SPSS version 12. Chi square test was used to compare proportions in 2x2 tables, while Fisher’s exact test was used for cells with small numbers. P value of < 0.05 was considered significant. Logistic regression was used to assess contribution of selected variables to survival beyond 24 hours after resuscitation. ResultsDuring the 6 month study period, a total of 1882 adult trauma patients were attended at the MOI casualty. Out of these, 67 patients (3.6%) had hemorrhagic shock and were eligible for the study. Twenty-two (32.8%) died on admission or during assessment before commencement of resuscitation and were excluded from the analysis. The remaining 45 patients were enrolled and resuscitated with 250 mls 7.5% hypertonic saline. Among the studied patients 36 (80.0%) were males and 9 (20.0%) were females. The median age was 28 years. Of the 45 patients 37 (82.2%) had been involved in a motor traffic accident, six were injured in a human assault, one had bullet injury and one was injured in a fall from a height. Of the studied population 64.4% had a single injury of which three quarters were visceral injuries. Sixty per cent of the patients had shock class III while 15.6% had class II and 24.4% had Class IV shock. Thirty-five patients (77.8%) had either no signs of head injury or a mild degree of head injury, the median Glasgow Coma score (GCS) being 15. Table 1 summarizes the characteristics of the study population. The SBP, DBP, MAP, and arterial oxygen saturation (SaO2) on admission were below normal in all patients. The mean rise of each after resuscitation was 38.30± 12.75, 24.04 ± 11.00, 25.96± 10.08 and 7.64% ± 6.95 respectively, and the change was statistically significant (p< 0.001). The pulse and heart rate dropped significantly by 25.89±8.65 and 26.02±9.30 respectively, a change that was statistically significant, p<0.001 On admission, the serum levels of sodium and chloride were within the normal range. Serum sodium concentration ranged from 130 – 145mmols/L with a mean concentration of 140.00 ±2.33 mmol/L. Serum chloride ranged from 97 – 111 mmol/L with a mean concentration of 106.22 statistically significant (p<0.001). Haemoglobin ± 3.40 mmol/L. After resuscitation, all patients and Haematocrit dropped significantly by mean had an increase in serum sodium and chloride drop of 1.51g/dL and 4.42% respectively concentration with mean rise of 10.96mmol/L and (p<0.001). 10.91mmol/L respectively. The increase was statistically significant (p<0.001). Haemoglobin and Haematocrit dropped significantly by mean drop of 1.51g/dL and 4.42% respectively (p<0.001). The level of consciousness improved after resuscitation with 7.5% HSS (Table 2 ). Among the studied patients, 88.9% recovered from shock immediately after being infused with 7.5% HSS. The proportion of those who recovered decreased with decrease in neither level of consciousness but neither age nor level of consciousness was statistically significantly associated with clinical recovery from shock. Of patients with a single injury, 96.6% recovered from shock whereas only 75% of those with multiple injuries recovered (p=0.047). Of patients with class II or III shock, 97.1% recovered from shock while only 63.3% of those with class IV recovered. This difference was statistically significant, p=0.01. (Table 3 ) Eighty percent of patients survived beyond 24 hours post resuscitation. Only 56.3% of those who sustained multiple injuries, survived beyond 24 hours while among those who had single injury, 93.1% survived beyond 24 hours. ( p = 0.006). The proportion of those with a severe form of shock (class IV) who survived beyond 24 hours was much lower than that of those with a lower class of shock. (p = 0.028) There was no association between the MAP, level of consciousness on admission with survival beyond 24 hours post resuscitation, p = 1.000 (Table 4 ) With logistic regression of baseline admission variables, age, type of injury and class of shock sustained were not predictors of survival beyond 24 hours after resuscitation. (Table 5 ) DiscussionThis study has demonstrated short term clinical benefits following administration of 7.5% hypertonic saline solution in patients with hemorrhagic shock. No adverse effects on homeostasis or haemodynamics were found. The goal of treatment of shock is to restore tissue perfusion and oxygen delivery. HSS infusion effects a rapid increase of blood volume, improves cardiac output, raises the blood pressure and therefore improves tissue perfusion.5,6,7 . The restoration of intravascular volume occurs at the expense of the intracellular volume compartment, therefore administration of regular intravenous fluid, and blood if required, should follow so as to eventually restore a normal fluid balance9. In the present study, rapid infusion of HSS caused a significant rise in systolic, diastolic and mean arterial pressure toward normal with a mean change of 38.30± 12.75, 24.04 ±11.00, 25.96 ±10.8, respectively (p<0.001). A rise in blood pressure improves cardiac output, which therefore improves tissue perfusion. The pulse and heart rate dropped significantly by 25.89±8.65 and 26.02±9.30 respectively. The patients had a sub optimal peripheral oxygen saturation before, which improved after resuscitation with a mean rise of 7.64 % ± 6.95, a rise which was statistically significant (p<0.001). HSS contains sodium and chloride at a concentration of 1,280 mmol/l. This is equivalent to nine times the normal serum sodium and 12 times the normal chloride concentration. Consequently, alterations of these serum electrolytes by a HSS bolus administration was given special attention in early studies to see if it would lead to complications. In the current series the only reported adverse effect was pain at the infusion site, documented in 5 patients (14.3%), all of whom had a change from gauge 16 to gauge 18 cannula. This may have been due to extravasation of the hypertonic fluid into surrounding tissue. Infusion site pain has not been reported in other studies. Of the numerous studies that have been carried out none has reported any clinical sign of hyperosmolarity5,6,7,20,23 . A few minor adverse effects, including restlessness, voiding urge, poor taste and vomiting were reported in one study 20 . They were more suggestive of reaction to very rapid infusion than to the temporary hyperosmolarity. No neuropathological signs were reported secondary to the relative hypernatremia. For patients who had an infusion of HSS and did not survive, autopsy done showed no evidence of central pontine myelinosis20 . In this study the mean serum sodium and chloride levels 5 minutes after HSS infusion was 151.91 ± 3.42 and 117.22 ± 4.27 respectively. Similar results were reported in previous studies. 6,20,23,26,27 More than 85% of the patients recovered from shock within the first five minutes after resuscitation with 250mls of HSS. More than 90% of the studied patients had an emergency operation soon after resuscitation. The short time required for infusion and the small amount of infusion (250mls of 7.5% HSS) to optimize these patients before anaesthesia is a great advantage in situations where life-saving surgery is urgently required and blood for urgent transfusion is not readily available. To attain the same degree of intravascular volume restoration with crystalloids would take close to 3 litres and a correspondingly long time to administer it. Eighty percent of the studied patients survived the first 24 hours. Different studies on HSS resuscitation have looked at its efficacy in improving survival by evaluating 24 hours and long-term survival. In these studies 24 hour survival rate was significantly higher in trauma patients who had an infusion of HSS as compared to isotonic saline. The survival rate ranged from 82.5% to 87.5%4, 7, 24, 25 . In conclusion, to the authors’ knowledge, this is the first study on small volume resuscitation in the East African region. It has demonstrated clinical benefits in initial treatment of traumatic hemorrhagic shock in patients admitted to the emergency room. The findings also indicate that side effects following small volume resuscitation with HSS are rare and generally without serious consequence. Small volume resuscitation with HSS is safe and effective. Clinical trials comparing the beneficial effects of HSS resuscitation with conventional isotonic fluids in the local setting are warranted. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07024t5.jpg] [js07024t2.jpg] [js07024t4.jpg] [js07024t1.jpg] [js07024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}