 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
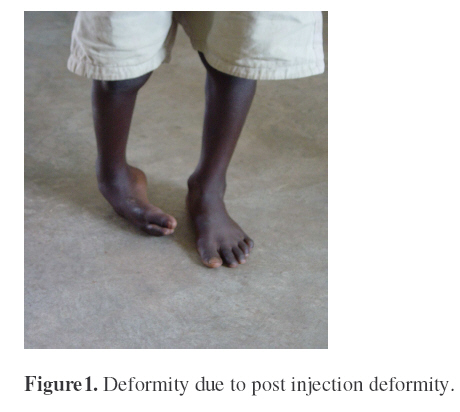
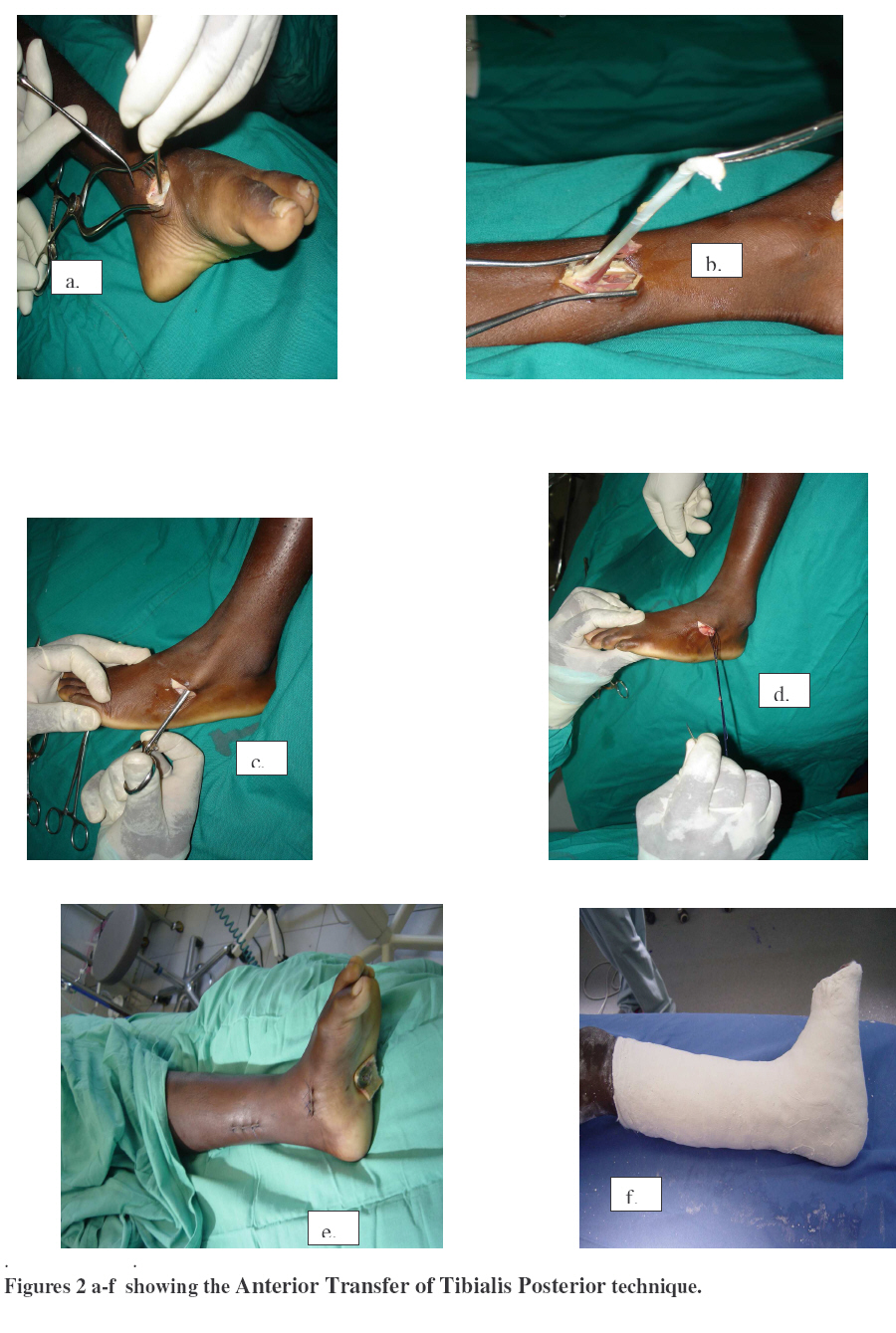
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 139-143 Anterior Transfer of Tibialis Posterior through the Interosseous Membranes in Post Injection Drop Foot: The Expirence at CORU. Okello, J.; Franceschi, F.; Loro, A.; Kintu, D. & Otim, I.CORU Mengo Hospital, Kampala, Uganda. Code Number: js07025 Post injection foot drop constitutes 7.6% of paediatric orthopaedic pathology seen in our unit. It commonly results from intragluteal injection with quinine in the treatment of malaria. The patients present with equinus or equinovarus foot deformity. Because of abnormal weight bearing, the deformity usually worsened with age. Anterior transfer of the tibialis posterior to the dorsum of the foot through the interosseous membrane has been described before and good results reported. The tendon is either transfixed by tenodesis to the cuneiform or cuboids. In our series the latter method was used. This is a follow up of 30 patients who had surgeries at least 18 months after the injection and muscles power of the tendon transferred ranged from 3 to 5. We used three incisions of approximately 4cm each instead of four. Postoperative plaster of Paris cast for 6 weeks and ankle foot orthosis were used. We evaluated for correction and ability of the transferred tendon to actively dorsiflex at the ankle joint. Nineteen patients had good results 8 fair and 3 poor there was no neurovascular deficit. The purpose of this paper is to outline our outcome and technique of anterior transfer of the tibialis posterior through the interosseous membrane. Introduction Post injection foot drop constitutes 7.6% of paediatric orthopaedic surgical pathology seen in our unit. It commonly results from sciatic nerve paralysis secondary to mechanical or chemical effects of intragluteal injection1. In our setting it is commonly due to injection with quinine in the treatment of malaria. The patients usually presents with equinovarus or equinus deformity because the dorsiflexors and evertors of the foot are most often paralysed. Occasionally the plantar flexors and suppinators are affected. Unlike in polio in which the toes are dorsiflexed, in post injection drop foot the toes are usually planter flexed. Since these children are rapidly growing, the abnormal weight bearing will deform the bone if not corrected early. In this study we focused on patients with equinovarus and varus deformity as illustrated below. Anterior transfer of tibialis posterior through the interosseous membrane to the dorsum of the foot is a standard orthopaedic procedure that has been utilized in the treatment of equinovarus foot deformity. Turner et al and Fried Independently described the procedure. The tendon can be transfixed to cuboid or cuneiform through a drill hole or transfix to the tibialis anterior2, 3 4 5 . Re-routing can be done through the interosseous membrane or anteriorly in the subcutaneous tissues. Usually four incisions are utilized when transferring through the interosseous membrane. Materials At Children’s Orthopaedic Rehabilitation Unit Mengo Hospital, we followed up 30 patients with 30 transfers because of equinovarus deformity secondary to post injection drop foot. The age at operation ranged from 3 to 12 years with an average age of 6. Patients with severe equinus deformity had equinus corrected percutaneously before tendon transfer; for equinus less than 10 degrees, fractional tendoachillis lengthening were done through the proximal incision during the transfers. Methods The purpose of this paper is to outline the outcome and technique of anterior transfer of tibialis posterior through the interosseous membrane to the dorsum of the foot in patients with equinovarus and varus deformity secondary to post injection drop foot who underwent the procedure in our unit. The power of the tendon transferred ranged from 3 to 5 and surgeries were done at least 18months after the onset of the paralysis. Surgeries were done under tourniquet applied to the thigh; three incisions of approximately four centimetres each are made. The first is made on the medial side of the foot through which we detach the whole tendon from it insertion, the second is at the level of musculotendinous junction where rerouting as well as fractional tendoachilislengthening in cases with equinus less than 10 degrees were done and lastly an incision is made over the cuboid. A tunnel is created with an artery forceps from the third incision to the second through interosseous membrane into which the tendon is passed. The membrane is perforated bluntly using an artery forceps, a hole is then drilled in the cuboid into which the tendon is fixed using a pullout vicryl suture fastened on a tuft and button on the plantar aspect. A post operative below knee plaster of Paris (POP) cast is applied with the foot in eversion and maintained for six weeks. After POP removal, an ankle foot orthosis is provided and used for six months; re-education of the transferred tendon is carried out during this period. ResultsThis was a crossectional study of 30 patients aged 3 to 12 years who had anterior transfer of tibialis posterior in Children’s Orthopaedic rehabilitation Unit Mengo Hospital from 2003 to march 2006 and the follow up period ranged from 6months to 3 years. We evaluated the feet for the ability of the transferred tendon to dorsiflex at the ankle joint, correction of dynamic deformity and prevention of recurrence. The evaluation was clinical with the patient walking towards and away from the examiner. We observe for position of the heel axis and weight bearing whether it is normal or on the lateral border of the foot during gait. The action of the transferred tendon was evaluated with the patient sitting and asked to actively dorsiflex at the ankle joint; the outcome were classified as good if there is correction of the equinovarus deformity and there is active dorsiflexion at the ankle joint; fair if there is correction of equinovarus but the transferred tendon is not active and poor if correction of the foot deformity and active movement are not achieved.
Twenty-seven (90%) of the patients had equinovarus deformities corrected. One patient developed calcaneovalgus, in this case the tibialis anterior regained the power and the transferred tendon was as well active; there were two cases of failed correction one of the patients was three year old at time of surgery, the transferred tendon was not active but tibialis anterior recovered partially. In twenty patients, the transferred tendons were active and in the remaining ten the tendon were not active this include the two cases with failed correction. Though ten patients had inactivity of the transferred tendon, eight had stabilizing effect in these cases the power of the muscles before transfer were three. Infection occurred in one case but sore at the site of buttons were common all this healed within three weeks. There was no neurovascular deficit in all DiscussionMuscles imbalance in children usually results into significant foot deformity due to abnormal weight bearing during the long period of growth. Since the deformity worsened with growth, transfer of a tendon helps in preserving function, and halting progression as well as correction of the foot deformity by restoring active dorsiflexion at the ankle joint as observed in this study. Nineteen of our patients had good results, 8 had fair results and 3 poor. There is usually residual weakness and wasting which depends on the degree of nerve injury. Bony procedure was not necessary since adequate correction achieved by tendon transfer only. The use of tibialis posterior as a dorsiflexor requires muscle re-education. A postoperative below the knee cast with the foot in eversion and dorsiflexion to reduce tension on the transferred tendon for six weeks is adequate for tenodesis has seen from our study and a similar duration of immobilization was reported before. Limited exposure did not affect the outcome in our series but this is significantly affected by power of the muscle before surgery. Muscles with power 4 and 5 before transfer had good outcome but those with power 3 had fair outcome. Although weaker muscles will not be active when transferred, the stabilizing effect that they provide to the feet helps in preventing equinovarus deformity but an ankle foot orthosis has to be worn for life. All patients in which equinovarus deformities were corrected had no recurrence. Poor results occurred in patients below five years this could be due to failure to know the exact duration of the paralysis resulting into surgery being performed at the time when the muscles are still in the recovery phase. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07025f3.jpg] [js07025f1.jpg] [js07025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}