 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
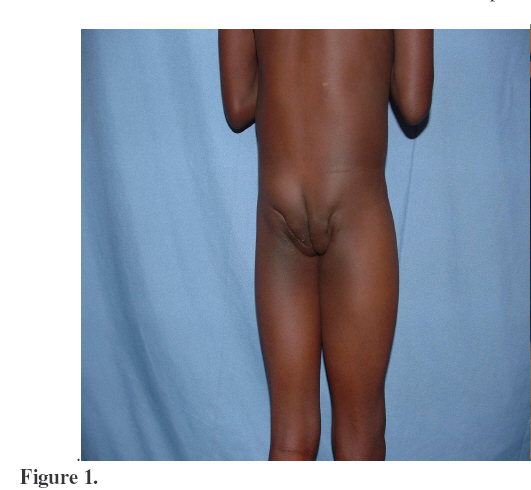
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 144-147 Gluteal Fibrosis. A report of 28 cases from Kumi Hospital, Uganda. Ekure, J. (MMed Orth Mak)Kumi Hospital, Uganda. Email: johnekure@yahoo.com Background: Gluteal fibrosis is a muscle disorder marked by intramuscular fibrous bands within the substance of the gluteal muscle. These bands lead to secondary contractures that affect the function of the hip joint(s). Different hypotheses have been put forward concerning the etiology of gluteal fibrosis. A congenital muscular dysplasia was postulated by Hnevkovsky10 and a lesion similar to the sternocleidomastoid muscle contracture in congenital tortocollis was suggested by Fairbank and Barret Llyoyd-Roberts and Thomas called attention because of severe systemic disease in infancy or childhood. Case reports Case 1. O.K., an 8 year old boy had difficulty in walking, squatting or sitting for six years following multiple injections of Quinine for treatment of malaria, on his buttocks at the age of 2 years, he was in fair nutritional status, a febrile, not anaemic and in the musculo-skeletal system, he had hip flexion in neutral limited to 30 degrees. External rotation and abduction of 35 degrees was necessary to obtain full flexion of the hips. No adduction or internal rotation was possible with the hips fully flexed. He squatted like a frog and sat with his lumber spine hyper flexed. He could not sit on a mat with his knees extended and hips abducted. Both buttocks were riddled with scars and were markedly wasted. Bilateral gluteal fibrosis release was done, as will be described and the patient had a full range of motion one month postoperatively. Table 1. Outcome of Surgery in 18 Patients with lteal Fibrosis.
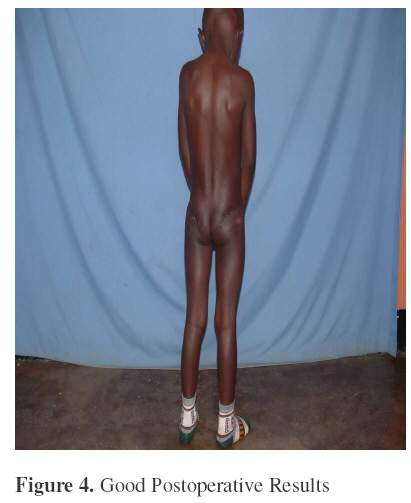
Ten more cases had a similar pattern above as in cases summarized in Table 1. Analysis of the cases:All the cases seen were children below the age of 12 years. Males constituted 44.4% of the cases seen. Malaria treated with IM Quinine was the commonest cause of the gluteal fibrosis. Other causes included PTB treated with Streptomycin and measles treated with IM Penicillin.In all the cases the child had small masses of the gluteal muscles and the buttocks were riddled with scars. Hip flexion in neutral was only possible to between 30 and 40 degrees in all patients and it was necessary to abduct and externally rotate the hips in order to obtain full flexion. When standing, the child kept an attitude of external rotation. Running was impossible because of the need to abduct and externally rotate the limbs at a very step. The condition was always bilateral. The child could not sit except in a high chair, then with a marked flexion of the lumbar spine. Squatting was difficult and only in frog position Pathological findings Macroscopically, a very tense fascia lata was found over the greater trochanter of every patient. The gluteus maximus and medius all appeared in most cases to be replaced by fibrous tissue. Some tissues could be described as ‘Plastic tissue’. Histology of this tissue showed intramuscular fibrosis without any sign of inflammation. TreatmentAll the 28 cases were operated up on. The Surgical procedure was as follows: An incision for the posterior approach to the hip was used. The dissection was carried out down to the deep aspect of the gluteus maximus, incising the fibrous tissue along the way. A transverse fasciotomy of the iliotibual tract was also done. Full and free hip flexion was determined to ascertain complete incisional release of the gluteal fibrosis. Only skin was closed and drain left insitu. Diathermy was always necessary for the procedure without which haemostasis would be a dream. The child was made to sit up within 48 – 72 hours and squatting exercises commenced as pain would allow, usually after five days. Our results were excellent and brought smiles to faces of many patients and parents. Three months after Surgery hip flexion averaged between 80 and 130 degrees. Two of our cases were complicated by sepsis and one developed paralytic foot drop Discussion:Different hypotheses have been put forward concerning the etiology of gluteal fibrosis. A congenital muscular dysplasia was postulated by Hnevkovsky and a lesion similar to the sternocleidomastoid muscle contracture in congenital tortocollis was suggested by Fairbank and Barret Llyoyd-Roberts and Thomas called attention because of severe systemic disease in infancy or childhood. In all of the reported cases of gluteal fibrosis, repeated intra muscular injections in the buttocks have been implicated 1,2,3,4,5,6. This is also true in our cases, and more so with the Quinine injections. The existence of scarred puncture marks on the buttocks was noted1,10 . None of our cases of gluteal fibrosis was diagnosed at birth, and therefore all of the cases reported here were secondary to mostly Quinine injections. Gluteal fibrosis is a preventable condition if proper administration of Quinine, mostly by IV route is emphasized. References.
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07026t1.jpg] [js07026f4.jpg] [js07026f2.jpg] [js07026f1.jpg] [js07026f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}