 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
East and Central African Journal of Surgery, Vol. 12, No. 1, April, 2006, pp. 148-153 Clinico-Surgical Outcome of Repair of Isolated Atrial Septal Defect At Care Hospital, Banjara Hills-Hyderabad India, 2004-2006. Ussiri1, E.V.; Mannam2, GopiChand; Sajja3 , Lokeswara Rao; Viswanath3, J.; Bhaskara Raju3, D.S.; Pathuri3, S.; Sompalli4, S.& Rao5 , N.K. 1Surgeon-Muhimbili National Hospital, Trainee-India, 2ChiefCardiothoracic Surgery CARE Hospital, Hyderabad-India, 3Consultant, Cardiothoracic Surgeon, CARE Hospital, 4Cardiac Anaesthesiologist & Critical Care, CARE Hospital, 5Cardiology, Paediatric Cardiology-Australia, Consultant Paediatric Cardiologist CARE Hospital Code Number: js07027 IntroductionAtrial septal defect (ASD) is the second commonest congenital heart disease accounting for 8% -13% following ventricular septal defects (1). ASD is classified into three major types which include ostium secundum, ostium primum and sinus venosus. Among all ASDs, ostium secundum account for 70%-80% 1,,2. Small defects, less than 5 mm diameter are asymptomatic and may decrease in size or close spontaneously whereas large defects, 12 mm or more they enlarge further3,4. Anita et al3 when evaluating 52 patients with secundum ASD in the first year of life with a follow-up of 2 – 3 years found that 46% of patients had decrease in the size of ASD with complete closure in 14 patients, 25 % the defects remained the same and 29% enlarged. Similar study was done by Mc Mahon CJ et al4 when evaluating the natural history of 104 patients with ostium secundum ASD revealed that the defects in 65% of patients increased in size and 4 % had spontaneous closure. The increase in size was attributed to the initial size of the defect rather than age at diagnosis. Small to moderate ASDs may remain asymptomatic till 4th decade of life while large defects may present early in life with heart failure, recurrent respiratory tract infection and failure to thrive3. Several studies revealed that surgical closure of ASD at young age have good outcome compared to those done in adults5,6,7 . Roos- Hesselink et al5 followed-up 135 patients after surgical closure of ASD to evaluate the long- term outcome results in terms of arrhythmias, pulmonary artery hypertension and left ventricle dysfunction for 21-33 years. It was concluded that ASD closure at young age, less than 11 years have excellent survival and low morbidity than when done at adult age. Similar results were obtained by Murphy JG et al6 when evaluating early repair of ASD in terms of sinus node dysfunction, atrial flutter or fibrillation, right ventricle dilatation, pulmonary artery hypertension and left ventricle dysfunction. Shah D et al7 did a comparative study on 72 patients with secundum ASD first diagnosed after the age of 25 years. The results concluded that there was no difference in survival or symptoms between those treated medically and those who underwent surgical closure. Also, the long-term outcome in terms of arrhythmias, stroke or emboli and heart failure was not improved by surgical closure.Retrospective study was done to evaluate the clinical presentation and outcome of the surgical closure of isolated ASD at CARE Hospital, Banjara Hills- Hyderabad, India. The aim of this study was to determine the clinical presentation and outcome of the surgical repair of isolated ASD. The Specific objectives were:
Patients and Methods Retrospective study for two and half years was done from January 2004 to June 2006 at CARE Hospital, Banjara Hills-Hyderabad India. Study included all patients who underwent surgical closure of the isolated ASD, either by direct suture or patch closure, both sexes and all age groups. Data were obtained from the Operating Room Registry and Medical Records and included age, sex, duration of symptoms, presenting symptom(s), intra-operative type of the defect, duration of ICU stay, duration of mechanical ventilation, duration and type of cardiac support used, development of atrial fibrillation, pre-and post-operative echocardiography findings, indications for cardiac catheterization where applicable, types of surgical techniques used and indications for patch closure, hospital stay and mortality. Data were analyzed using Epi-info 6 program for statistical significance. Echocardiography Definitions:
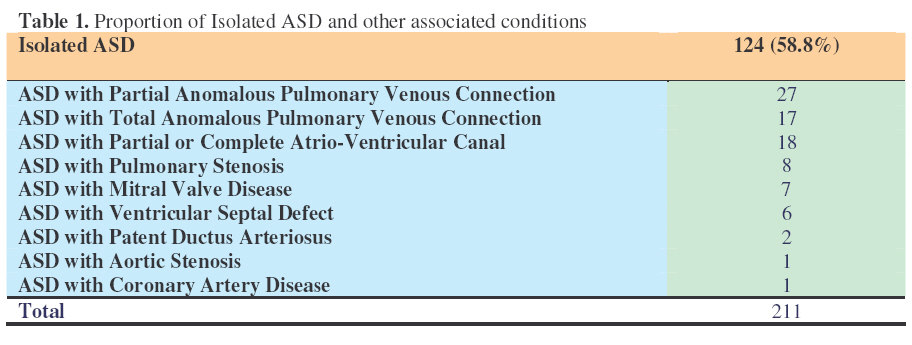
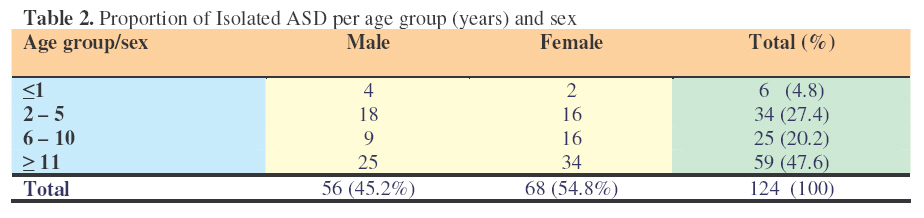
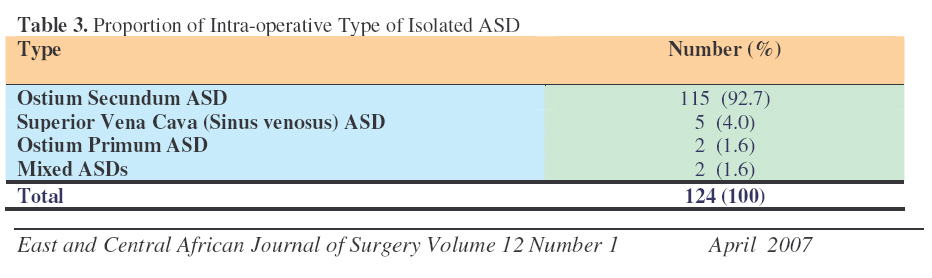
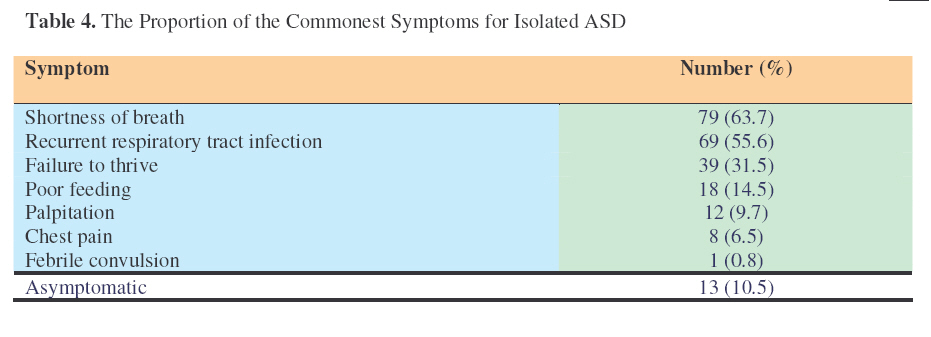
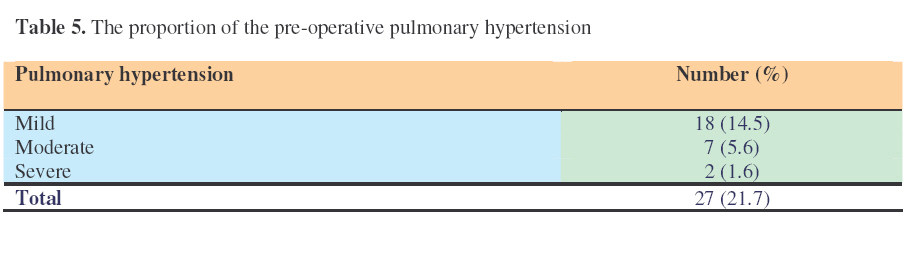
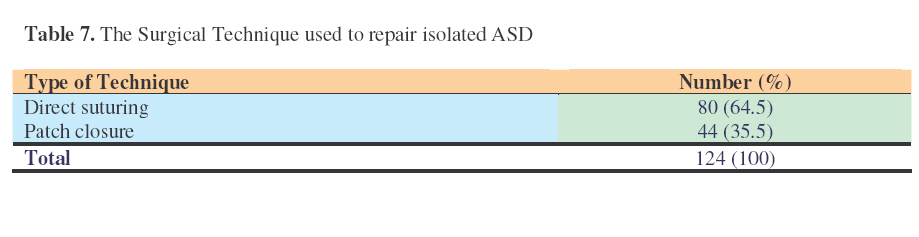
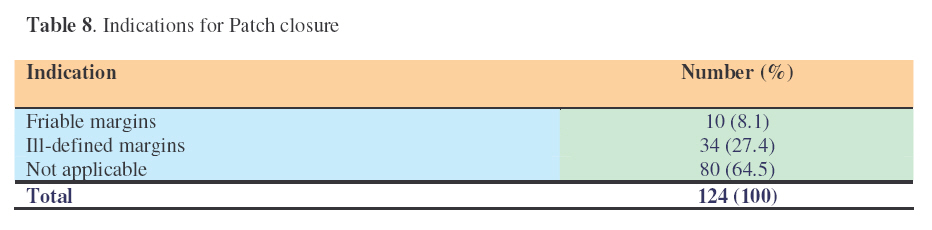
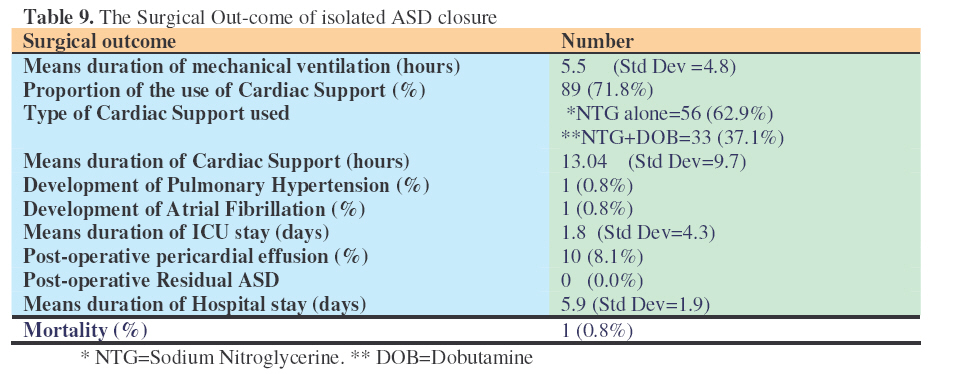
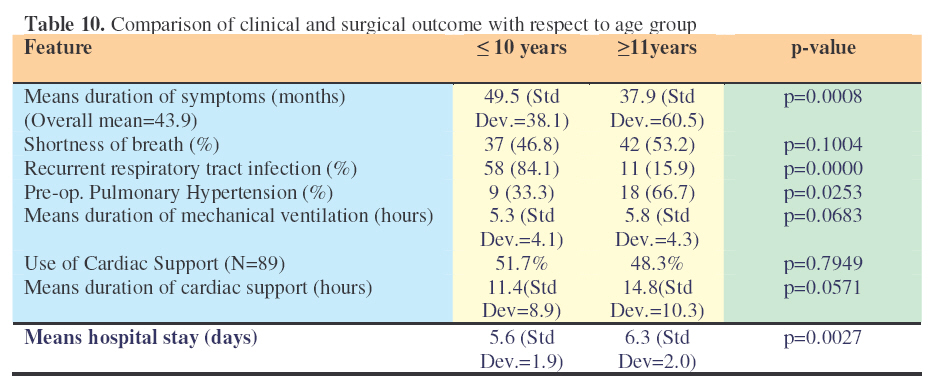
Results The study revealed a total of 124 (58.8%) patients with an isolated ASD. The other associated conditions commonly included anomalous pulmonary venous connection, atrio-ventricular canal, pulmonary stenosis, mitral valve disease and ventricular septal defect (Table 1). Females had higher predominance than males and ostium secundum was the commonest type of ASD accounting for 92.7% (Table 2 & 3). The commonest symptoms included shortness of breath, recurrent respiratory tract infection, failure to thrive and poor feeding in children Among 124 patients, only 14.5% had cardiac catheterization done for preoperative assessment while the rest were diagnosed by clinical examination and echocardiography only. Surgical repair for these defects included direct suturing (64.5%) and 0.5% glutarldehyde treated autologous pericardial patch (35.5%). Pericardial patch closure was applied for defects with friable margins and ill-defined margins including one patient with common atrium. The surgical outcome for these patients revealed a mean duration of mechanical ventilation of 5.5 hours (Std Dev. = 4.2), 71.8% of all patients were maintained on a post operative cardiac support with a mean duration of 13.0 hours (Std Dev. = 9.7). Commonly used cardiac supports included NTG alone (45.2%) and a combination of NTG and Dobutamine (26.6%). Mean duration of ICU stay was 1.8 days (Std Dev. = 4.3) and mean duration of hospital stay was 5.9 days (Std Dev. = 1.9). Mild to moderate post-operative pericardial effusion was observed in 8.1% of the patients and this recovered spontaneously. One patient with severe post-operative pulmonary hypertension was managed medically with oral Sildenafil, Milirinone, NTG, Sodium Nitroprusside and Frusemide with good recovery. Mortality rate was 0.8% in this study for one patient who was 45 years old developed atrial fibrillation and low output syndrome on the third post-operative day. The necessary resuscitation measure, cardiac supports and expertise consultation were done but patient died of multiple organs failure on the eleventh post-operative day. When comparing the clinico-surgical outcome between the age-group 10 or less and above 11 years it was found that there was a significant difference in the means duration of symptoms, 49.5 months (Std Dev.=50.1) vs. 37.9 months (Std Dev.=60) respectively, (p=0.0008), significant proportion of recurrent respiratory tract infection, 84.1% vs. 15.9% respectively(p=0.0000) and significant mean hospital stay 5.6 days (Std Dev.=1.8) vs. 6.3 days (Std Dev.=2) respectively (p=0.0027). Clinically and statistically the incidence of preoperative pulmonary hypertension was increasing with age significantly (33.3% vs 66.7% respectively, p= 0.0253). Tables 3, 4, 5, 6, 7, 8, 9, and 10 Discussion The study revealed that females had higher predominance than males and ostium secundum was the commonest type of ASD accounting for 92.7%. Similar results were obtained by the other studies1,2,8 . Adult patients presented with palpitation, shortness of breath and chest pain. Anita et al3 found the similar symptoms. Cardiac catheterization is only indicated in patients with ASD to evaluate severe pulmonary artery pressure, left heart function and haemodynamics, co-morbid anomalies, coronary artery for patients above 40 years or for percutaneous closure of ostium secundum ASDs9. Echocardiography is the primary imaging modality used in the evaluation of ASDs because of its high sensitivity and specificity, low cost and easy accessibility10 . The necessary resuscitation measure, cardiac supports and expertise consultation were done but patient died of multiple organs failure on the eleventh post-operative day. The above findings were similar to other studies8,11,12,13,14,15 . Clinically and statistically the incidence of preoperative pulmonary hypertension was increasing with age significantly (33.3% vs 66.7% respectively, p=0.0253). There was no significant difference between the two groups in terms of mean duration of mechanical ventilation, use of cardiac support, mean duration of cardiac support and ICU stay. Several studies2,5,6,7,8,13,16,17 concluded that surgical repair of ASD has a good outcome when done during childhood than in adults in terms of atrial fibrillation, thromboembolic phenomena, left ventricle systolic function, degree of mitral and tricuspid valve regurgitation.
Special thanks to the Administration of CARE Hospital, Banjara Hills, Hyderabad-India for allowing this study, Mr. Sashidhar DSL and Mrs Jhansi J of Records Department-CARE Hospital, all staffs of Old Cardiothoracic theatre and ICU and Mr. Mayunga F of Muhimbili University College of Health Sciences, Department of Epidemiology and Biostatistics for statistical analysis. References
© 2007 East and Central African Journal of Surgery The following images related to this document are available:Photo images[js07027t5.jpg] [js07027t10.jpg] [js07027t9.jpg] [js07027t4.jpg] [js07027t8.jpg] [js07027t1.jpg] [js07027t2.jpg] [js07027t3.jpg] [js07027t7.jpg] [js07027t6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}